The “Crush” procedure is a 2-stent technique for the treatment of bifurcation lesions with greater rates of in-stent restenosis than the Culotte technique. In conclusion, we report a possible mechanism for this discrepancy in the case of severe Crush stent fracture with associated focal restenosis identified by postmortem microcomputed tomography and histologic examination.
Percutaneous treatment of coronary bifurcation lesions is technically challenging and associated with an increased risk of complications, including in-stent restenosis. Although a single-stent strategy is preferred, a 2-stent strategy, such as the Crush or Culotte technique, is frequently required. As a part of our routine autopsy protocol, we identified a Crush-treated bifurcation lesion with severe stent fracture identified in the main branch (MB) and side branch (SB) stents with associated restenosis identified on microcomputed tomography and histologic examination.
Case Report
A 67-year-old man with known coronary artery disease died of cardiogenic shock secondary to an anterior myocardial infarction. Three years before his death, percutaneous coronary intervention was performed to treat crescendo angina and lateral ischemia found on stress testing. Cardiac catheterization at that time revealed a Medina class 1,1,1 left circumflex/first obtuse marginal (OM1) bifurcation lesion that was treated by deploying a 2.5 × 18-mm sirolimus-eluting stent (Cypher, Cordis, Bridgewater, New Jersey) in the OM1 and then a 3.5 × 18-mm sirolimus-eluting stent in the left circumflex artery across the OM1 branch using the Crush technique ( Figure 1 ). Coronary angiography 3 years later demonstrated subtotal occlusion of the OM1 SB ( Figure 2 ).


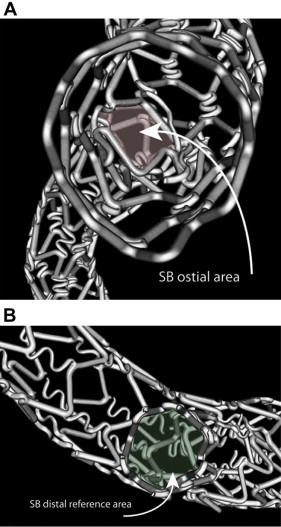
At autopsy, the heart was explanted and pressure fixed with 10% formalin, and the coronary arteries were perfused with bismuth/gelatin contrast. The stented arterial segment was then resected under fluoroscopic guidance and scanned with microcomputed tomography (GE LocusSP, London, Ontario, Canada) at 23-μm resolution. The data were then processed (Analyze, version 9.0, Rochester, Minnesota) to generate 2- and 3-dimensional reconstructions for examination of restenosis and stent fracture. The proximal first crown of the 2.5-mm stent deployed in the OM1 SB was crushed against the vessel wall by the 3.5-mm left circumflex MB stent ( Figure 3 ). All the flexible N-shaped linker segments between crowns 1 and 2 of the SB stent were fractured. Adjacent to the carina, the MB stent had fracture of most of the flex segments connecting the 3 to 4, 4 to 5, and 5 to 6 crowns ( Figure 3 and Video 1 ). The ostium of the SB was created by struts from the MB and SB stents, creating an ostial area stenosis of 37% relative to the distal SB ( Figure 4 ). The area of greatest restenosis in the SB and MB stents was near the region of flex segment fracture ( Figure 5 ). Histologic examination confirmed subtotal occlusion at the ostium of the OM1 branch ( Figure 6 ).