Bronchial sequelae of a foreign body. Anteroposterior chest x-ray of a 5-year-old child presenting with chronic atelectasis in the left inferior lobe (a). Axial CT scan of the chest, showing bronchiectasis in the left lung (b)
Radiological Study
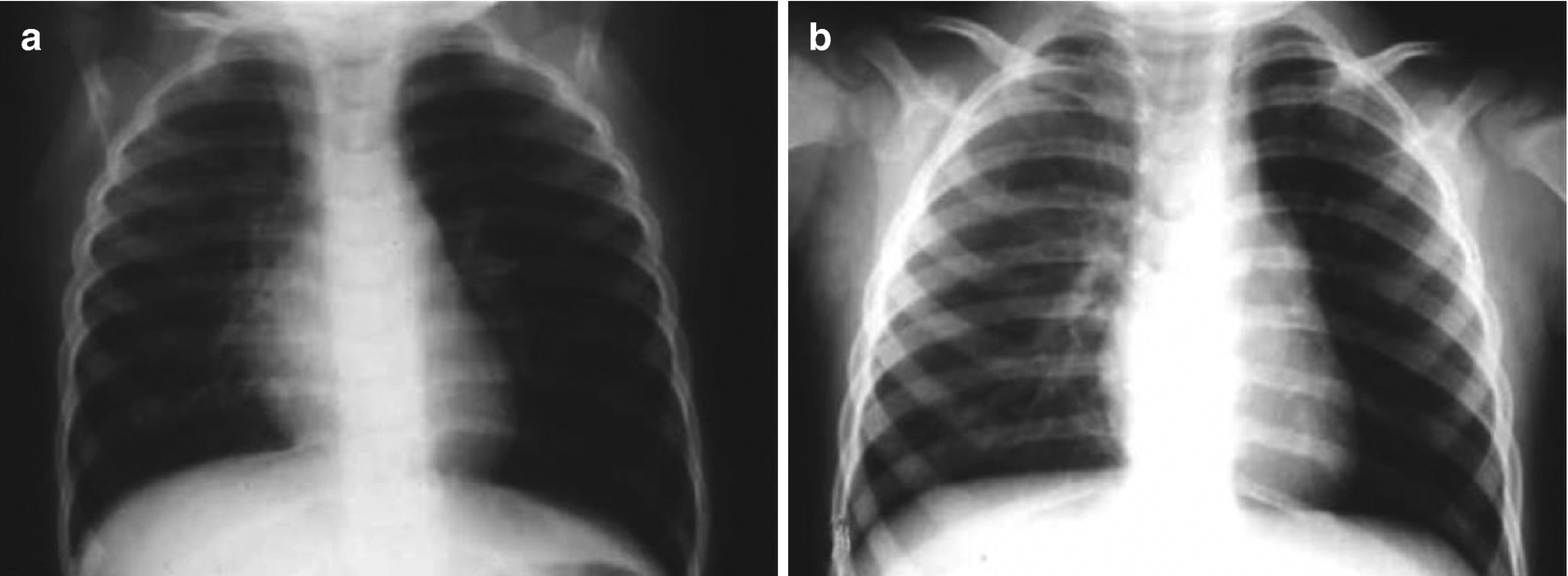
Lung hyperinflation. Anteroposterior chest x-rays of a 4-year-old child during inhalation (a) and during exhalation, showing hyperinflation of the left hemithorax (b)

Radiotranslucent foreign body in the left source bronchi, with secondary left lung hyperinflation
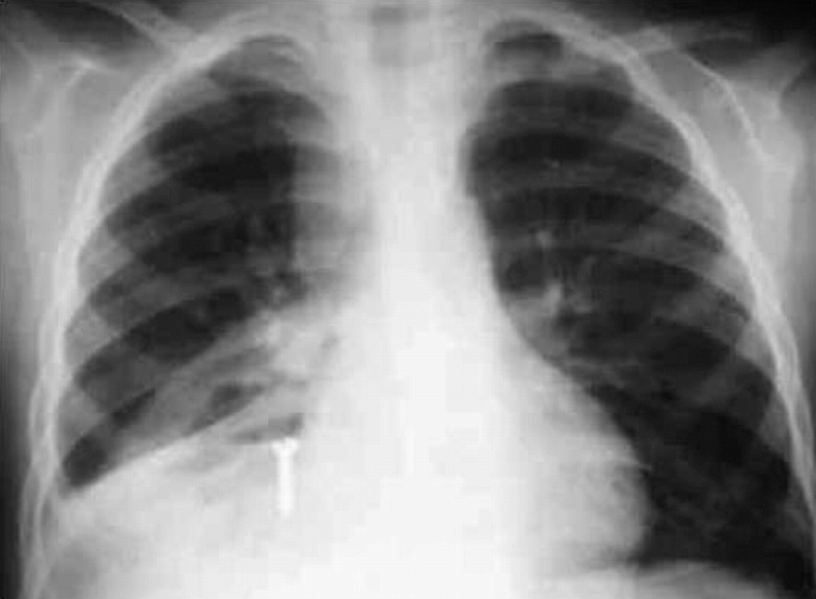
Radiopaque foreign body (a screw) in the right posterior basal bronchi
If the foreign body remains in the bronchi for an extended period, radiography may show atelectasis or bronchiectasis, the extent of which depends on the level of interlocking.
The usefulness of computerized tomography (CT) and virtual endoscopy is debatable. It has been suggested that these are indicated in cases of penetration syndrome with normal radiography, to avoid the anesthesia required for rigid bronchoscopy. However, in these cases, fiber bronchoscopy evaluation under sedation is more advantageous than CT, which, in addition to involving a radiation dose and being less readily available, also does not show the nature of the foreign body or the presence of granulation tissue, and thus has no therapeutic value.
Treatment
Immediate action in response to penetration syndrome can result in dislodgement of the foreign body. In an infant, this involves slapping the child’s back while he or she is being held with his or her head downward, with or without chest compression. In an older child, the classic Heimlich maneuver can be performed.
Treatment in response to inhalation of a foreign body is based on endoscopic extraction. There is no consensus as to the best anesthetic protocol, but there is more support for having the patient pharmacologically paralyzed than for maintaining spontaneous ventilation.
The most universal therapeutic approach is based on the degree of certainty about the presence of the foreign body.
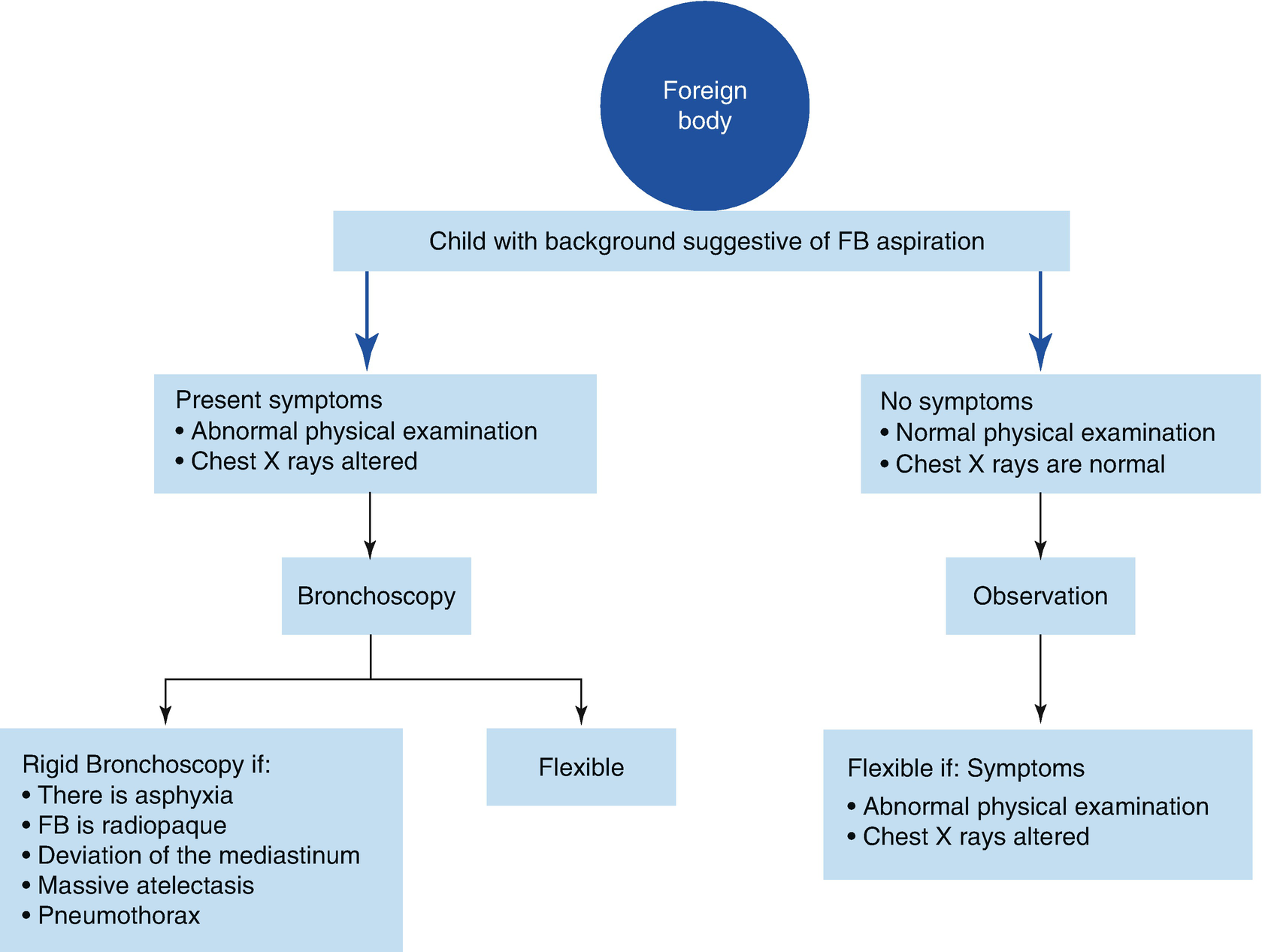
Absolute certainty: There is absolute certainty in the case of dyspnea or persistent coughing after penetration syndrome, with asymmetry on pulmonary auscultation, localized hyperinsufflation, or a radiopaque foreign body. In these cases, the use of therapeutic bronchoscopy is indicated. Most often, the clinical situation is stable because the foreign body is located in the bronchi; thus, removal can wait for the recommended fasting time and to ensure the availability of the ideal equipment for extraction. On the other hand, extraction is urgently required if there is severe respiratory distress, mediastinal diversion, massive atelectasis, a pneumothorax, or, in the case of a particularly harmful foreign body such as a battery, because it can cause tissue necrosis, or spikes, that rapidly migrate distally.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


