The neck represents a unique, compact unit of multiple life-supporting structures, all of which must be addressed and treated if injured. Vascular injuries of the neck make up approximately 5% of all civilian vascular injuries but should take the highest priority when evaluating patients with cervical trauma once an airway is secured. Like most trauma, these vascular injuries can occur with both penetrating and blunt mechanisms. Unlike most other trauma, however, penetrating wounds make up the vast majority (approximately 95%) of the potentially significant injuries seen in a major urban trauma center. As the end organ of all cervical arteries is the brain, arterial injuries in the neck cannot be considered to be the same as extremity arteries that supply musculoskeletal organs only.
General Information
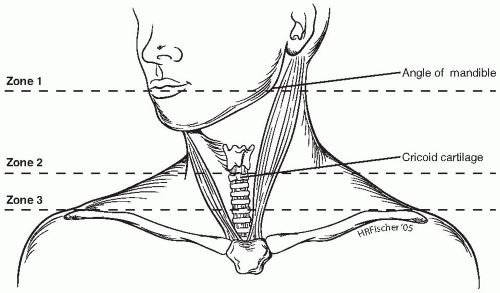
Overall, gunshot wounds represent the most common mechanism of injury in cervical neck trauma. Some series examining these injuries, however, have an equal or greater number of patients with stab wounds versus gunshot wounds. In these papers, approximately two-thirds of all penetrating wounds to the neck occur on the left side, secondary to the preponderance of right-handed people inflicting this trauma. The common carotid artery is the most often injured of the major vessels, followed by the internal carotid and external carotid. Overall, the mortality has been reported to range from 2% to 10%, depending upon the mechanism of injury, other associated injuries, and time between injury and presentation to a trauma center. Patients presenting with profound neurologic central deficits carry a high mortality, although the majority of deaths occur due to other associated injuries. Classically, all penetrating injuries to the neck have been described by their location in one of three zones as first suggested by the Cook County Hospital experience in 1969. Zone 1 was described as being below the sternal notch, zone 2 between the sternal notch and angle of the mandible, and zone 3 above the angle of the mandible. This classification is still used today, with the usual modification of including those injuries up to the level of the cricoid cartilage as being in zone 1 (Fig. 78-1).
Historic Overview
Although attempts to treat acute cervical vascular injuries took place as far back as Ambroise Pare in the 1500s, the first useful experience with penetrating neck injuries occurred during the large-scale military conflicts of the 20th century. An early series reported 124 carotid injuries during World War I, all treated with ligation for active hemorrhage. This resulted in approximately 30% of patients having a stroke. Ligation for bleeding remained the mainstay of treatment through World War II, although carotid artery injuries represented only a small fraction (10/2471) of all the arterial injuries reported. During the Korean conflict, the first attempts were made to repair arterial injuries of the neck rather than do simple ligation. One series reported 11 carotid injuries out of 304 total vascular injuries (3.6%), of which four were repaired using direct transverse suture, primary anastomosis, and placement of an interposition vein graft. These reports from military conflicts initially brought the treatment of vascular trauma to the forefront, where it could be examined and studied in a scientific way.
Figure 78-1. Illustration of the three zones of the neck used by most trauma centers. Zone 1 encompasses that region from the clavicle to the cricoid cartilage. Zone 2 is from the cricoid to the angle of the mandible. Zone 3 includes the region from the angle of the mandible to the base of the neck.
During the 1950s, the first nonmilitary reports concerning penetrating vascular injuries to the neck were published. In the first reported major review, 100 penetrating neck injuries that were surgically explored revealed 11 major arterial injuries, 8 minor arterial injuries, and 30 major venous injuries. This high rate of positive findings led to the recommendation that all penetrating injuries traversing the platysma should be explored. This paper also documented that the mortality of those explored in less than 6 hours was 4%, versus 20% in those explored after 6 hours, thus demonstrating a profound effect of prompt treatment on outcome. These findings and recommendations were later confirmed in other studies. The dogma of mandatory surgical exploration continued for more than 2 decades, until advances in technology offered alternative approaches. Concurrently, the entire field of vascular surgery came into its own as early vascular pioneers reported their experience with successful use of bypasses, endarterectomies, and other basic surgical techniques.
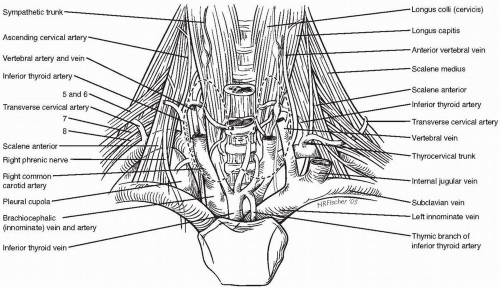
Figure 78-2. Illustration of the anatomy at the base of the neck showing the important arteries, veins, and nerves.
Today, in the early 21st century, obvious vascular injuries manifesting hard signs are still treated for the most part as they were years ago with immediate open exploration. The main controversies now evolve around the diagnosis and management of cervical vascular injuries with no hard signs. With the ever-changing advances in technology, the modern surgeon must keep abreast of what has been tried before and what new techniques hold real promise for the future. Continuing education in the field is a must to determine when modern technology is advantageous to the surgeon and when standard, proven methods for approaching these injuries better apply.
Penetrating Trauma
Pertinent Anatomic Features
Anatomic and technical differences when operating in the neck first led physicians to define three different zones, or areas, in which a penetrating missile traverses. Initially, zone 1 was defined as below the clavicle, but injuries proximal (or caudal) to the clavicle are better considered to be thoracic or mediastinal injuries and addressed in that manner. Penetrating injuries superficial to the platysma or in the posterior muscular triangle are considered inconsequential, as no major vascular or aerodigestive structures occupy these regions.
The carotid arterial system carries 90% of the blood flow to the brain. The intracranial collateral circulation varies widely, with a complete circle of Willis present only 20% to 50% of the time. This results in the trauma patient being highly susceptible to ischemic injury when an acute occlusion occurs to either carotid artery. Other collateral systems, such as the external carotid-ophthalmic, occipital-vertebral, and leptomeningeal vessels that may develop over time in chronic occlusive disease, have little benefit in the acute trauma situation. Figure 78-2 demonstrates the anatomy of the lower neck. The common and internal carotid arteries lie within the carotid sheath, medial to the internal jugular vein, anterior to the vagus nerve, and they usually give off no extracranial branches. The external carotid artery typically has eight major branches, the first being the superior thyroid artery and the terminal branch being the palpable superficial temporal artery. The carotid sinus is a baroreceptor located at the flow divider of the carotid bifurcation. When stimulated, it causes a reduction in the heart rate and blood pressure. The adjacent carotid body is a chemoreceptor responsive to carbon dioxide and will cause an increase in the heart rate and blood pressure when stimulated. Generally, extensive dissection of the carotid bifurcation between the external and internal carotid arteries should be avoided in order to maintain proper function of these structures (Fig. 78-3).
The vertebral arteries arise as the first branch of the subclavian arteries bilaterally (Fig. 78-3). The first segment extends from the subclavian to where it enters the transverse process of the sixth vertebral body. The second segment (longest) lies in the foramina of the transverse processes of the first six vertebrae. The artery is surrounded by a venous plexus that often lends itself to forming AV fistulas following penetrating trauma to this segment. The third segment is short and lies between the atlas (C1) and the foramen magnum at the base of the skull. The fourth segment is intracranial and ends when the two vertebral arteries join together to form the basilar artery of the posterior system. Approximately 15% of patients will demonstrate developmental abnormalities resulting in a unilateral hypoplastic vessel. Another 4% to 5% will lack direct communication of one vertebral with the contralateral side.
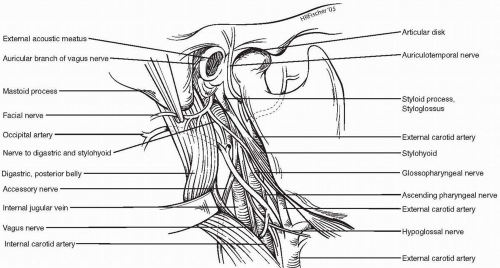
Figure 78-3. Illustration of the anatomy of the upper half of the anterior neck.
Associated Injuries
Associated injuries are common and should be evaluated separately from potential arterial injuries. The most common associated injury is that to adjacent major veins, occurring in approximately 25% to 30% of cases. Tracheal or laryngeal injuries are found in 9% to 10% of penetrating neck trauma, esophageal or pharyngeal injuries are found in 4% to 5%, and spinal cord or brachial plexus injuries occur in 1% to 2%. Signs and symptoms of these injuries include dysphagia, vomiting, hemoptysis, subcutaneous emphysema, shortness of breath, and enteric contents draining from the wound. Studies have shown a 60% to 80% chance of a positive finding on surgical exploration if crepitance, hoarseness, and stridor are present. Asymptomatic patients with missiles traversing the midline near the aerodigestive tracts should undergo bronchoscopy and an esophagram or high-resolution computed tomography (CT) scan of the neck.
Injuries to the cranial nerves and other important nerves of the neck can occur from both the traumatic event and surgical exploration. It is important to thoroughly evaluate and document each patient for neurologic deficits prior to initiating treatment. The major nerves often injured in the neck, their location, and their resulting deficits are listed in Table 78-1.
Table 78-2 gives a good overall perspective concerning all possible injuries seen in 110 patients with bullet wounds to the neck. Careful auscultation and x-ray of the chest need to be performed in all penetrating neck trauma, as thoracic abnormalities (pneumothorax +/− hemothorax) requiring tube thoracostomy are the most frequently encountered associated injuries. Generally, a CT scan of the head is also needed (especially in zone 3 injuries) to delineate intrinsic cerebral trauma versus neurologic symptoms secondary to vascular compromise. Any clinical evidence of spinal injury should also warrant a CT scan of the bony neck for definitive evaluation. Associated injuries are a leading cause of death in patients with neck trauma, directly resulting in a mortality rate of 2% to 8%.
The base of the neck is the second most commonly injured zone. Patients presenting with hard signs of vascular injury and hemodynamic instability should be taken directly to the operating room for exploration, based on the projected path of the missile and most probable site of injury. Hard signs of arterial injury of the neck are listed in Table 78-3. Although amenable to physical examination in some injuries, extreme care must be taken to assure that significant vascular trauma has not occurred just beneath the bony structures in patients with penetrating zone 1 injury. Unlike the other two zones, there is general agreement that some diagnostic measure must be undertaken when confronted with these injuries and no hard signs. Classic teaching recommended arteriography in these circumstances to fully delineate the extent and exact location of vascular injuries. Studies have shown the missed injury rate to be 1% or less, with a complication rate in the 1% to 2% range. (See Fig. 78-4.)
Table 78-2 Associated Injuries Seen with 110 Bullet Wounds to the Neck
Injury
# Patients
(%)
Pneumothoraces/hemothoraces
30
27.2%
Venous injuries—major
18
16.4%
Mandibular fractures
18
16.4%
Long bone fractures
12
11.0%
Cervical spine injury
9
8.2%
Arterial laceration—major
7
6.4%
Abdominal wound requiring surgery
7
6.4%
AV fistula
7
6.4%
Esophageal laceration
7
6.4%
Skull fracture
6
5.5%
Thoracic spine injury
6
5.5%
Brachial plexus injury
6
5.5%
Laryngeal laceration
6
5.5%
Salivary duct laceration
3
2.7%
Facial nerve injury
2
1.8%
Sinus perforation
2
1.8%
Only gold members can continue reading. Log In or Register to continue