We have read with great interest the report by Merchant et al recently published in The American Journal of Cardiology . The investigators address an issue that has attracted much interest over the past year, that of early repolarization (ER) being linked to sudden cardiac arrest due to malignant ventricular arrhythmia.
Merchant et al sought to identify electrocardiographic (ECG) features to distinguish benign from malignant variants of ER. They retrospectively analyzed QRS notching or slurring in 9 patients with ER plus idiopathic ventricular tachycardia or ventricular fibrillation (VF) compared with those of a group of 200 healthy controls with ER. The investigators noted that QRS notching was more common in leads V 4 and V 5 in patients with idiopathic VF than in controls, and there was a similar tendency in lead V 6 for the 2 groups. These results do not agree with those of Rosso et al who, in a similar study, reported that J-point elevation in leads V 4 and V 6 was equally frequent in patients with VF and controls but more frequent in the inferior leads, leads I and aVL, in the patients.
However, there are several technical aspects that the investigators of the 2 studies do not report in ECG method, which may have a decisive influence on their mutually contradictory results. In the following paragraphs, we comment on the importance of ECG filtering and signal sampling for the interpretation and comparison of ECG tracings.
Electrocardiographic Filtering
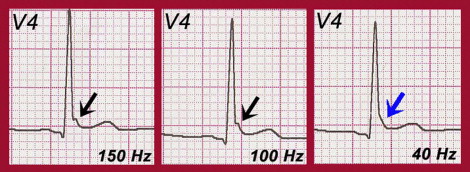
It is of paramount importance to consider what filter parameters are applied in ECG acquisition, because they may distort or alter the original cardiac signal. Specifically, the application of a low-pass filter with a low cutoff is a common mistake in clinical practice. Although this type of filtering attenuates high-frequency artifacts, such as muscle noise, it also eliminates or attenuates the meaningful signals that were the subject of this study, such as the J wave or its manifestation in the form of notching ( Figure 1 ). It must be noted that a significant proportion of the controls presented QRS slurring; some could be due to low-pass filtering with a low cutoff. In that case, the results could be very different.
Type of Electrocardiographic Device: Filter Order and Signal Sampling
Merchant et al selected electrocardiograms with ER obtained from 1988 to 2008. During the 20-year study period, the technology evolved. Although all ECG devices must meet certain standards and be validated for use in clinical practice, there may be differences between them (in terms of signal processing, analog-to-digital conversion, and printout). Thus, electrocardiograms obtained using ECG devices from different manufacturers may vary, despite being from the same patient and obtained with exactly the same electrode placement.
It must also be borne in mind that there may be differences between ECG signals obtained with different models, even when using the same cutoff frequency, because the filter order is not necessarily the same, especially if the equipment is from different manufacturers.
A basic parameter is the sampling frequency of the signal that the device uses. A sampling frequency that is too low can have a significant effect on many high-frequency components of the electrocardiogram, such as the notches that occur within the QRS complex. A minimum sampling frequency of 500 Hz is needed to reproduce all the measurable high-frequency components.
We congratulate Merchant et al on addressing this interesting line of research on the ECG features of ER in patients with idiopathic VF, but we believe that the omission of technical details directly affecting ECG morphology makes it difficult to assess their results and conclusions.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


