(1)
Department of Neuroscience, University of Turin Ospedale Molinette, Turin, Italy
Abstract
The embryological evolution of the venous system of the brain has been treated largely by many authors (Streeter 1918; Hochstetter 1938; Padget 1956, 1957; Kaplan and Ford 1966; Okudera et al. 1984; Raybaud et al. 1989). We summarize the essential points.
The embryological evolution of the venous system of the brain has been treated largely by many authors (Streeter 1918; Hochstetter 1938; Padget 1956, 1957; Kaplan and Ford 1966; Okudera et al. 1984; Raybaud et al. 1989). We summarize the essential points.
The veins develop in a later stage in comparison to the arteries. In the early stages of the embryogenesis the venous drainage is characterized by a superficial network draining into a superficial dural plexus, formed by an anterior, middle and posterior parts, on either side, which drains into the paired Primary Head Sinus (PHS) continuing posteriorly in the Anterior Cardinal Veins (future Internal Jugular Veins). From the anterior part of the plexus, arises the Primitive Marginal Sinus which continues caudo-ventrally, in the Primitive Tentorial Sinus. Later, the PHS regresses, with exception of its anterior part, from which develops the cavernous sinus. The anterior middle and posterior components of the Dural Plexus fuse together on the midline, forming the Superior Sagittal Sinus, continuing in the Torcular Herophili and further in the now formed Transverse – Sigmoid sinuses. From these dural complex arises progressively the superficial venous system, including the cortical veins collecting the blood from the pial and medullary veins.
The deep venous system appears later. It is characterized by choroidal, diencephalic veins and by a large median venous channel known as the median prosencephalic vein (PV) (Markowski 1922) or as primitive internal cerebral vein (Padget 1956, 1957). These veins drain the blood of the well-developed choroid plexus into the Primitive Marginal Sinus directly or through a primitive straight sinus. The development of the basal ganglia and thalamus results in the formation of the paired internal cerebral veins which replace the primitive diencephalic veins and the PV and annex also the venous drainage of the choroid plexus acquiring progressively the typical horizontal sinuous course. In the meantime many tributaries of the internal cerebral vein develop forming the subependymal and deep medullary veins. The drainage of these veins is centripetally directed. Differently, the flow of the superficial medullary veins is centrifugally directed toward the superficial system. The development of the internal cerebral veins leads progressively to regression of the PV with exception of its more distal part which together with the distal segments of the internal cerebral veins forms the Galen vein draining in the straight sinus.
The straight sinus is displaced posteriorly acquiring in the newborn its oblique caudally directed pattern. In addition to the straight sinus, another primitive dural channel can be present called the falcine sinus. It normally disappears. It can, however, be incidentally discovered during normal examinations (Sect. 9.3.3). It is frequently the main venous drainage of Galen vein malformation (Sect. 12.8) often associated with hypoplasia – aplasia of the straight sinus.
As far as the basal vein is concerned, it is a vessel formed by the fusion of primitive pial vessels represented by the telencephalic, diencephalic, and mesencephalic venous channels. This explains the presence of the several tributaries entering the final basal vein coming from the cerebral hemispheres and brainstem. In the early stage of this evolution, the primitive pial veins are connected also with the primitive tentorial sinus, which later, due to the posterior expansion of the brain parenchyma, extends dorsally reaching the transverse sinus. The connection of the primitive pial veins with the tentorial channel normally disappears, but occasionally remains, explaining the drainage of the final basal vein into this dural channel. Commonly, however, the basal vein extends posteriorly and medially entering the Galen vein.
Considering the embryogenesis of the veins of the posterior fossa, the early appearing veins are the anterior vein draining the anterior part of the brainstem and the posterior vein draining the cerebellar structures. In the early phases, the anterior is the most voluminous and will be involved in the formation of the petrous vein, its tributaries, and the superior petrosal sinus. The posterior vein is first smaller, since, in this phase the cerebellum is not yet completely developed. Later, in connection with the growth of the cerebellum, a group of veins develops, draining in the transverse or straight sinuses. A partial part of the drainage of the posterior fossa will be enclosed in the Galen vein (Sect. 9.2).
Considering the embryological development of the veins, this is characterized by many variations, due to changes involving the morphology, flow direction, and development of various connections, and so the pattern is not so constant in comparison to that of the arteries. Nevertheless, some typical aspects can be always recognized. We will describe the veins of the supratentorial area and those of the posterior fossa (infratentorial) and the pattern of the dural sinuses with their tributaries.
9.1 Supratentorial Cerebral Veins
The supratentorial cerebral veins can be subdivided into the superficial and deep systems (Kaplan and Ford 1966; Salamon and Huang 1976). The first drains the blood toward the superior sagittal, the transverse, the sigmoid, and the cavernous sinuses and the second into the internal cerebral and basal veins continuing in the Galen vein and straight sinus.
9.1.1 The Superficial System
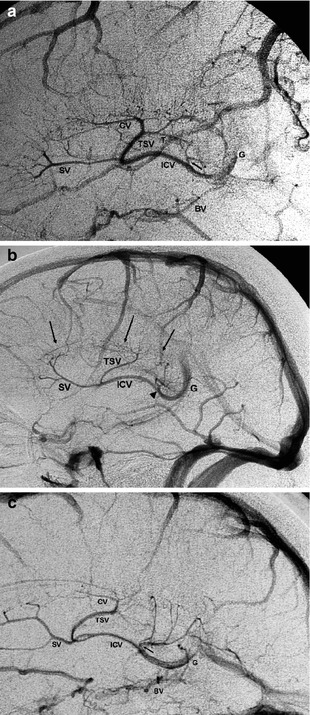
This comprises the cortical veins draining the cortex and superficial medullary veins, which drain the more superficial white matter. The medullary veins run in a centrifugal direction toward the cortex, where they join the cortical veins. The latter run within the subarachnoid space along the superficial sulci, frequently crossing the gyri. Close to the sinuses, they perforate the arachnoid and dura, where they run through their internal layers before entering the sinuses (Figs. 9.1, 9.4, 9.5, 9.7, 9.8, and 9.10).
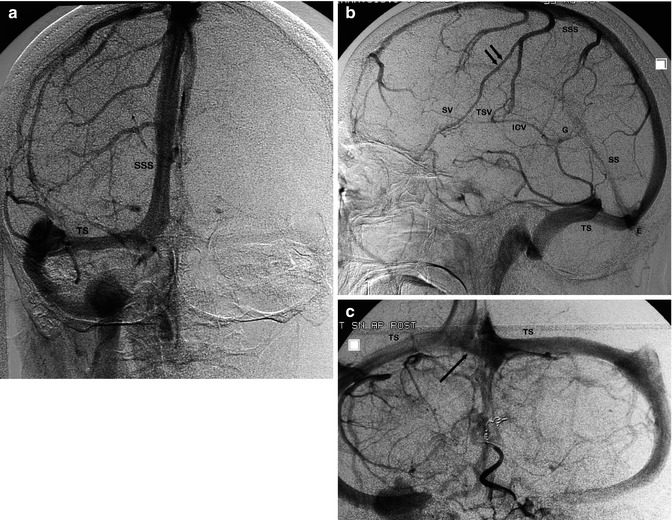
Fig. 9.1
Carotid angiogram, anteroposterior (AP) and lateral view. Venous phase (a, b). The SSS drains predominantly into the right TS. Among the cortical veins entering the SSS, there is a large Trolard vein (double arrow). Thalamostriate vein (TSV), septal vein (SV), internal cerebral vein (ICV) with its typical S-shaped course, vein of Galen (G), straight sinus (SS), torcular herophili (E). Vertebral angiogram (c) in the same patient. On this angiogram is documented the presence of the left TS, in which drains predominantly the SS. There is a complementary dural channel connecting the right and left TS at the torcular herophili (arrow) (patient treated for distal PICA aneurysm, with occlusion also of the distal PICA with coils)
9.1.1.1 Superior Group
The veins of this group have an ascending course entering the superior sagittal sinus (SSS). The group includes the veins of the lateral surface of the fronto-parieto-occipital lobes, part of the veins of the medial surface of the hemispheres (Sect. 9.1.1.4), and those of the anterior part of the orbital surface of the frontal lobe. The posterior part of the frontobasal area drains in the system of the basal vein (see Sect. 9.1.2.7). Sometimes a vein called the vein of Trolard (Fig. 9.1) connecting the SSS with the superficial middle cerebral vein is present. The flow can predominate toward the SSS, and so the superficial middle cerebral vein can be small or absent or vice versa. The veins are well recognizable on the AP and especially on the lateral carotid angiogram. In the frontal area the veins enter the SSS at a right angle. The more posterior veins join the sinus, forming a progressively more oblique angle in the direction against the flow of blood into the SSS (Figs. 9.1, and 9.5) (Oka et al. 1985).
9.1.1.2 Anterior–Inferior Group
The main vein in this group is the superficial middle cerebral vein (SMCV) (Figs. 9.5a–d, 9.6, and 9.10) which collects several branches of the lateral inferior surface of the frontal and parietal area and from the lateral superior surface of the temporal lobe. It can be single or represented by a group of veins.
The SMCV runs along the surface of the sylvian fissure and continues into the sphenoparietal sinus (see also Sect. 9.3.9). This latter enters the cavernous sinus or it can run directly toward the base of the skull, where it divides into small channels that pass through the foramina of the base, reaching the pterygoid plexus. This variant is called paracavernous drainage (Wolf and Huang 1963) (see also Sects. 9.3.9, 9.3.10, and Fig. 9.21). The SMCV can drain directly into the cavernous sinus or having a paracavernous drainage, in those cases, where the sphenoparietal sinus is absent or poorly developed (San Millan Ruiz et al. 2004; Tubbs et al. 2007b). In another type of drainage, the SMCV runs around the floor of the middle cranial fossa reaching the superior petrous sinus or continuing in the tentorial sinus toward the transverse sinus. The SMCV can anastomose with a large temporal vein forming the vein of Labbè, which is a venous channel running on the surface of the temporal lobe draining posteriorly into the transverse sinus (Hacker 1968, 1974). This latter can be the predominant drainage when the SMCV is small or absent (Figs. 9.4 and 9.6).
As far as it concerns the deep middle cerebral vein and the veins of the insula, see Sect. 9.1.2.7.
9.1.1.3 Postero-inferior Group
The veins of this group also called the tentorial group drain the lower lateral and the lateral basal surface of the temporal and occipital lobes. These veins converge to the lateral tentorial sinus which is an intratentorial venous channel entering the transverse sinus (Oka et al. 1985). More rarely the veins drain directly in the transverse sinus or converge in a large vein of Labbé.
9.1.1.4 Veins of the Medial Surface
The veins of the medial frontoparietal surface run upward, curve over the superior margin of the hemisphere where they connect with the veins of the lateral surface, and together enter the SSS. The lower part of the medial surface close to the cingulated gyrus, the cingulated gyrus itself, and the corpus callosum drain, in the frontal area, into the anterior pericallosal vein and into the posterior pericallosal vein (splenial vein) in the parietal area (Salamon and Huang 1976; Oka et al. 1985). The drainage can occur partially also in the inferior sagittal sinus (ISS). As far as it concerns the medial surface of the occipital lobe, the drainage occurs through the anterior calcarine vein (also called internal occipital vein) entering the posterior pericallosal vein (splenial vein), sometimes the basal vein, and through the posterior calcarine vein draining into the SSS (Oka et al. 1985).
The anterior pericallosal vein is a paired vein which courses around the genu of the corpus callosum and further in the cisterna of the lamina terminalis reaching the anterior cerebral vein tributary of the basal vein (Fig. 9.2). Sometimes the anterior pericallosal vein can run upward entering the ISS. The posterior pericallosal vein is a paired vein, sometimes a single vein which runs in the pericallosal cistern around the splenium entering the vein of Galen and sometimes the basal or internal cerebral vein (Ben-Amor and Billewicz 1970; Duvernoy 1975; Salamon and Huang 1976).
9.1.2 The Deep System
The deep system drains the blood centripetally from the deeper white matter, including that of the corpus callosum and internal capsule, and from the deep structures of the gray substance (basal ganglia, thalamus, septum pellucidum, fornix, and claustrum) into two main collectors: the internal cerebral vein and basal vein. To this system belong the medullary veins, the subependymal veins, the veins of the basal ganglia, the internal capsule, the claustrum, the thalamic veins, and the choroidal vein (Figs. 9.2, 9.3, 9.5, 9.6, 9.7, 9.8, and 9.9).
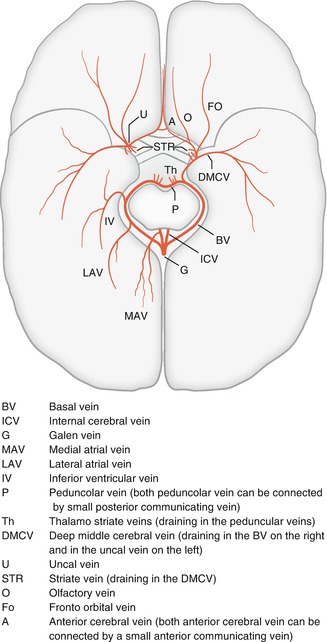
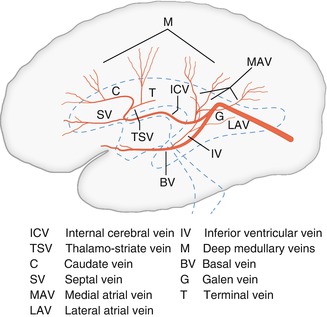
Fig. 9.2
The basal vein and its tributaries seen from below
Fig. 9.3
Lateral view of the deep cerebral veins
9.1.2.1 Medullary Veins
These veins originate in the deep white matter and run toward the lateral ventricle, where they enter the subependymal veins (Huang and Wolf 1964; Wolf and Huang 1964). The deep and superficial medullary vein can anastomose, forming a continuous venous channel that extends from the cortex to the subependymal veins (Schlesinger 1939; Kaplan 1959). On the lateral carotid angiogram, the medullary veins especially those in the frontal and parietal regions are frequently well visible as very fine vessels, which are directed centrally with an oblique or perpendicular course, before joining the subependymal veins (Figs. 9.3, 9.6, and 9.9).
9.1.2.2 Subependymal Veins
The subependymal veins derive their blood from the medullary veins and from the basal ganglia, septum pellucidum, fornix, and corpus callosum of each hemisphere (Wolf and Huang 1964; Salamon and Huang 1976). Some of these veins are relatively constant; the presence of others can be very variable. We describe the most typical.
The septal vein (SV, vein of the septum pellucidum) arises each from several tributaries characterized by deep medullary veins in the frontal region, converging to the anterior lateral corner of the frontal horn. The SV runs further to the medial corner; it then turns backward, continuing into the two sleeves of the septum pellucidum, joining the internal cerebral vein at the foramen of Monro. It can have an anomalous course (anomalous SV), running in the superior part of the septum pellucidum, turning then downward, and reaching the internal cerebral vein behind the foramen of Monro (Figs. 9.1, 9.3, 9.6, 9.7, 9.9, and 12.17c–f).
The thalamostriate vein (TSV) is usually prominent among the subependymal veins. It is formed by the junction of the terminal vein, which runs beneath the stria terminalis between the thalamus and the body of the nucleus caudatus, and the caudate veins draining the nucleus caudatus. Among the caudate veins, the anterior caudate vein is frequently the larger. Sometimes, the caudate veins drain more posteriorly, reaching the internal cerebral vein directly through a vein called the direct lateral vein, which courses horizontally across the floor of the lateral ventricle. The TSV joints the internal cerebral vein together with the SV at the foramen of Monro or near to it (Salamon and Huang 1976). Despite its name, the TSV does not drain the thalamus (Giudicelli et al. 1970; Salamon and Huang 1976) (Figs. 9.1, 9.3, 9.5, 9.6, 9.7, 9.8, and 9.9).
Among other subependymal veins, we briefly describe the atrial veins and inferior ventricular vein. The medial atrial veins (MAV) and lateral atrial veins (LAV) receive tributaries from the medial and lateral walls of the atrium and occipital horn. The tributaries of the MAV run anteriorly, converging to a stem, which enters the internal cerebral vein near the Galen vein (Figs. 9.2, 9.3, and 9.9). The LAV is rarer (Figs. 9.2 and 9.3). Its tributaries run more inferiorly, reaching the distal segment of the basal vein or inferior ventricular vein (IVV).
The IVV (Figs. 9.2, 9.3, and 9.6) begins in the body of the lateral ventricle, accompanies the body and tail of the nucleus caudatus, and runs anteriorly in the roof of the temporal horn, forming an anterior concave curve. It exits to the choroid fissure, entering the basal vein. Several tributaries reach the vein, in particular those from the hippocampus and adjacent temporal areas.
9.1.2.3 Veins of the Basal Ganglia, Internal Capsule, and Claustrum
The superior part of these structures drains by the way of the superior striate veins into the subependymal veins (see Sect. 9.1.2). The inferior part drains into the inferior striate veins, which run downward and pass through the anterior perforate space, reaching in the deep portions of the sylvian fissure the stem of the deep middle cerebral vein, which is a tributary of the basal vein (Wolf and Huang 1963; Salamon and Huang 1976). They are rarely recognizable on an angiogram (Fig. 9.8).
9.1.2.4 Thalamic Veins
These veins are divided into the superior, inferior, anterior, and posterior groups. The superior group has the largest draining vein, which runs first parallel to the internal cerebral vein, entering then its posterior part. The inferior group emerges at the posterior perforated substance, reaching the peduncular vein (tributary of the basal vein). The anterior group drains into the internal cerebral vein (ICV) near the foramen of Monro and the posterior group into the basal vein (Giudicelli et al. 1970; Salamon and Huang 1976) (Figs. 9.12 and 9.13). They are visible in the venous phase of the vertebral angiogram.
9.1.2.5 Choroidal Veins
The choroidal plexus is drained by the superior and inferior choroidal veins; their tributaries are, respectively, the ICV and the basal vein (BV) (Ben Amor et al. 1971; Salamon and Huang 1976). The superior and inferior choroidal veins belong to the subependymal veins, but they receive blood only from the choroidal plexus and are recognizable on an angiogram as a faint blush in the capillary phase.
9.1.2.6 Internal Cerebral Vein
The ICV is a paired venous channel, arising at the level of the foramen of Monro or near to it. It is located near the midline, where it runs in the tela choroidea on the roof of the third ventricle.
Each vein arises as a junction of the SV with the TSV and receives during its course several subependymal veins. Each ICV ends in the cistern of the quadrigeminal plate, below the splenium, where both veins unite and, together with both BV, enter the vein of Galen. The ICV is always recognizable on the lateral carotid angiogram owing to its typical S-shaped form and in the anteroposterior (AP) view owing to its paramedian position.
The ICV and some of its tributaries (SV, TSV) are a constant venous finding. They are better demonstrated on the later lateral angiogram when the cortical veins slowly disappear (Figs. 9.1, 9.4, 9.5, 9.6, 9.7, 9.8, 9.9, and 9.10). The SV appears later differently from ICV and TSV which are filled earlier. On the AP view commonly only the ICV and the TSV are well recognizable (Figs. 9.4, 9.5, 9.6, 9.7, and 9.8). As far as it concerns the other deep veins, overlapping variations and different filling make it not possible their certain identification in every case. The situation is different when these veins are dilated, like in the drainage of vascular malformations (Figs. 12.8, 12.9, and 12.12).
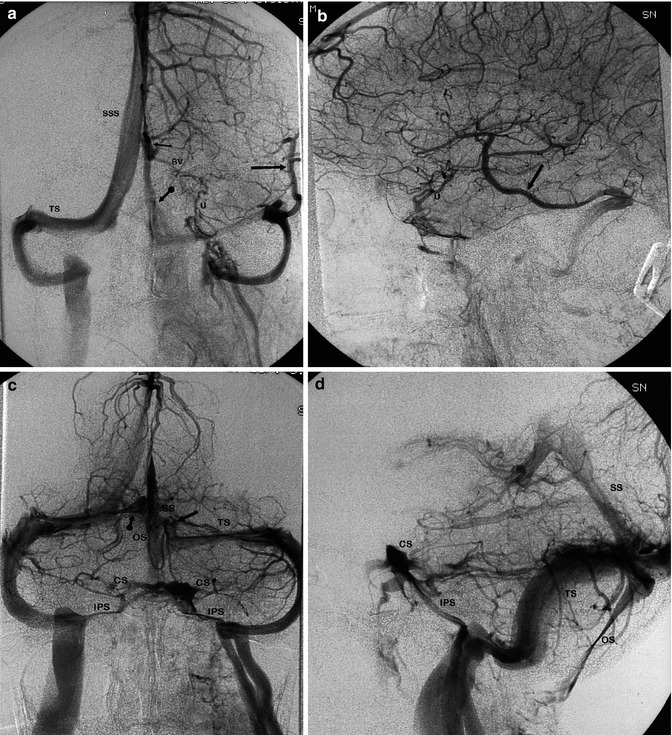
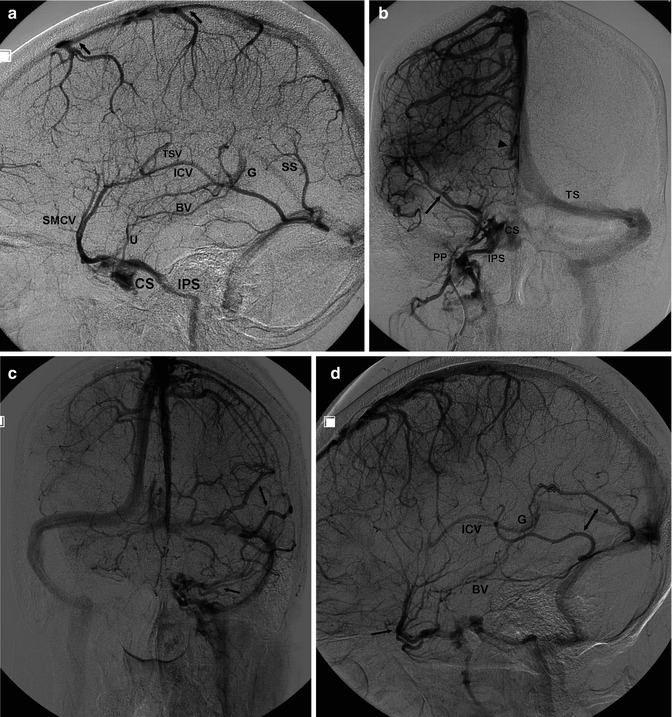
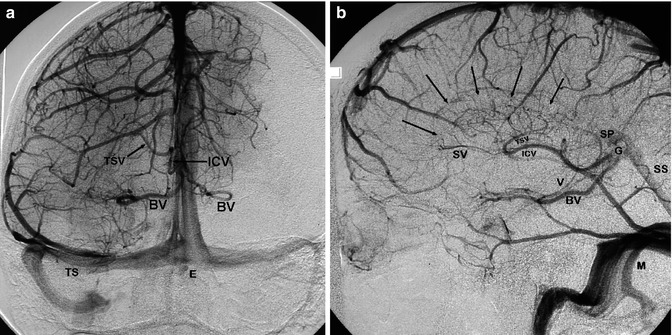
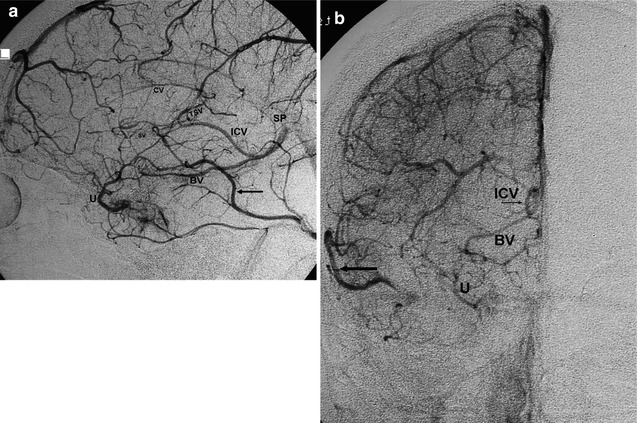
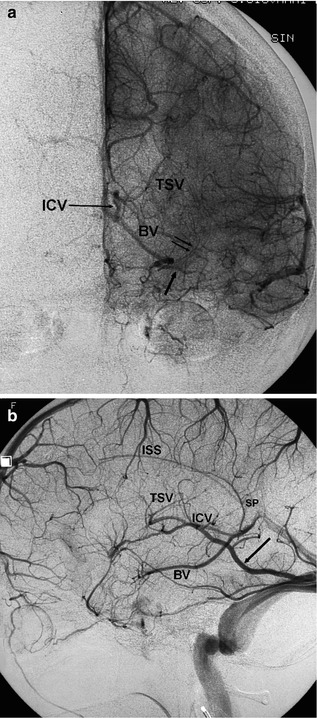
Fig. 9.4
Carotid angiogram, AP and lateral view, venous phase (a, b). The SSS drains into the right TS. The left TS is partially injected through the straight sinus (arrow with dot). There is a large vein of Labbé (arrow) draining into the distal part of the left TS. Large uncal vein (U) receiving blood from the anterior tributaries of the basal vein (BV). Typical paramedian course of internal cerebral vein (arrow) receiving its tributaries. Vertebral angiogram in the same patient, AP and lateral view, venous phase (c, d). Better filling of the straight sinus (SS) and of the left TS. There is a complementary venous channel to the TS (arrow). There is also a connection (arrow with dot) with the right TS. There is a large occipital sinus (OS) connected posteriorly with the SS and TS. Inferior petrosal sinus (IPS), cavernous sinus (CS)
Fig. 9.5
(a) Carotid angiogram, venous phase, lateral view. There is a large superficial middle cerebral vein (SMCV), draining into the cavernous sinus (CS) and further in the inferior petrosal sinus (IPS). There is a small uncal vein (U), draining partially the anterior tributaries of the basal vein (BV). Internal cerebral vein (ICV), thalamostriate vein (TSV). The septal vein is not recognizable; it appears frequently in later venous phases. Vein of Galen (G), straight sinus (SS). Typical course of the cortical veins, draining into the SSS with from frontal to occipital a progressively reverse direction to the flow of the sinus. (b) AP view in a different patient. ICV (arrowhead). The duplicated SMCV (large arrow) drains into venous channels located lateral to the CS. The lateral venous channels correspond partially to the “paracavernous sinus” and to the “lateral cavernous sinus,” both draining into the pterygoid plexus (PP). Rich anastomoses (small arrow) connect these channels with the CS which continues into the IPS. There is no injection of the right TS. The drainage of the SSS occurs into the left TS. (c, d) AP and lateral views in another patient. AP view: the venous drainage of the temporal lobe occurs through a complex SMCV with several branches (arrow) entering the CS. The further drainage continues into the IPS and partially into the pterygoid plexus. The posterior part of the temporal lobe is drained by two large channels (bidirectional arrow) entering the TS. The SSS drains into the right TS. The left TS drains the temporal veins and the deep venous system through the Galen vein–straight sinus. Lateral view: same indications. Internal cerebral vein (ICV), Galen vein (G), small basal vein (BV)
Fig. 9.6
AP (a) and lateral (b) angiograms. Venous phase. There is a bilateral injection of the cortical frontal vein and basal vein (BV). In the late venous phase visible on the lateral angiogram, there is a faint network (arrows) corresponding to the medullary veins draining into the subependymal veins (ICV, TSV, SV). There is also an injection of the inferior ventricular vein (V) with its typical anterior concave curve, to which converge fine branches of the lateral atrial vein. Splenial vein (SP), vein of Galen (G), straight sinus (SS). There is no superficial middle cerebral vein. The drainage of the temporal lobe occurs through a large basilar vein and two large temporal veins entering the TS after a short intratentorial course. Mastoid emissary vein (M). There is duplication of SSS in two channels, well recognizable in the AP view; the smaller one is divided further. All these channels enter the torcular herophili (E)
Fig. 9.7
Lateral (a) and AP (b) angiograms, venous phase. Part of the anterior tributary of the basal vein (BV) drains anteriorly into the uncal vein (U), which ends in the cavernous sinus. Internal cerebral vein (ICV). There is a very long caudate vein (CV). Thalamostriate vein (TSV), small septal vein (SV), splenial vein (SP), basal vein (BV). There is no SMCV. The drainage of the temporal region is directed prevalently into the vein of Labbé (arrow), into the large frontal and parietal veins and into a tentorial channel entering the TS
Fig. 9.8
Lateral (b) and AP (a) view of the carotid angiogram, venous phase. Basal vein (BV). In the AP view, its tributaries, represented by the deep middle cerebral vein (arrow) collecting the inferior striate veins (double arrow), are visible. There is a small superficial middle cerebral vein, while drainage of the temporal region occurs prevalently into the large temporal vein (Labbé) toward the TS (large arrow on lateral angiogram). Internal cerebral vein (ICV) collecting thalamostriate vein (TSV). Splenial vein (SP). Presence of the inferior sagittal sinus (ISS). The septal vein is not visible in this venous phase; it appears later. This angiographic finding is not rare. Indeed, the septal vein drains mainly the white matter and not the gray matter, and so its circulation time is prolonged
9.1.2.7 Basal Vein (BV)
First described by Rosenthal (1824), the BV is an important, frequently large vein, collecting blood from the supratentorial and infratentorial veins. It is formed on the undersurface of the anterior perforated substance (APS) by the union of several veins (Fig. 9.2). In most cases, the deep middle cerebral vein (DMCV) is the most important tributary, and so the BV appears as its direct continuation (Duvernoy 1975). The DMCV is formed by several veins running on the surface of the insula, directed inferiorly and anteriorly toward the pole of the insula (Wolf and Huang 1963). It runs further medially in the deep portion of the sylvian fissure, where it is joined by the inferior striate veins. At the level of the APS, the DMCV is connected with the other tributaries of the BV, which are the veins of the frontobasal region (olfactory and frontoorbital veins) and the anterior cerebral vein. This latter receives blood from the rostrum and the genu of the corpus callosum by way of the anterior pericallosal vein, continuing to the vein of the lamina terminalis, which enters the anterior cerebral vein (see also Sect. 9.1.1.4). Both the anterior cerebral veins are linked by the anterior communicating vein, running above the optic chiasma (Duvernoy 1975; Ono et al. 1984).
From its point of origin, the BV runs along the base of the brain, around the cerebral peduncle medially and the uncus laterally, forming an S-shaped curve. The posterior cerebral artery lies inferiorly while the anterior choroidal artery crosses the BV superiorly from medial to lateral. In its more distal segment, the BV runs slightly upward along the posterior side of the thalamus to join the vein of Galen or the ICV (Figs. 9.2 and 9.3).
The BV receives along its course many tributaries. Near its origin there are the peduncular veins which run in the interpeduncular fossa, draining the inferior thalamic veins. The peduncular veins of both sides are connected to each other by a small communicating vein (Duvernoy 1975; Salamon and Huang 1976). Other tributaries are the inferior ventricular vein (IVV) and the lateral atrial vein which have already been described (Sect. 9.1.2.2). The BV drains also the veins of the inferomedial temporal lobe, the veins of the medial anterior part of the occipital lobes, and sometimes the posterior pericallosal vein which is also called splenial vein (see also Sect. 9.1.1.4). Another vein that can be connected with the BV is the lateral mesencephalic vein, which runs in the lateral mesencephalic sulcus and can be also connected with the petrosal vein, forming an anastomosis between the supratentorial and infratentorial venous sectors (Wolf et al. 1963; Bradac 1970; Wackenheim and Braun 1970; Salamon and Huang 1976).
Many variants have been described (Padget 1957; Bekov 1965; Babin 1971; Duvernoy 1975; Salamon and Huang 1976): one is represented by the posterior mesencephalic vein, which arises from the mesencephalon and runs to the vein of Galen. It can replace the BV or may be present in addition to it. In the latter case, Duvernoy (1975) proposed that it should be called the accessory basilar vein. The distal segments of the BV can be absent, and so the proximal segments drain infratentorially through the lateral mesencephalic vein into the petrosal vein. In other cases, the first segment does not anastomose with the more distal, and so the first tributaries, mainly the DMCV and frontal veins, join to form a common trunk (uncal vein), which usually drains into the cavernous or paracavernous sinus (Figs. 9.4, 9.5, and 9.7). Rarely, the BV can drain posteriorly into the transverse or straight sinus (SS) after a short course within the tentorium (Johanson 1954; Padget 1956; Wolf et al. 1963; Duvernoy 1975).
On an angiogram, the BV is well recognizable in the lateral view as a venous channel, forming a slight upwardly concave curve in its course to the vein of Galen. In the AP view, the main trunk forms a small curve corresponding to the peduncular vein before showing a straight, medially directed course toward the vein of Galen. The presence and recognition of its tributaries are irregular.
In contrast to some subependymal veins (ICV, SV, and TSV), which are always recognizable with a typical pattern, the BV, in its normal course, is not always present owing to the above-described variants. The BV and the posterior mesencephalic vein can have the same pattern on an angiogram. Furthermore, the same vessel may be differently filled depending on the injection of its tributaries, which can differ on carotid and vertebral angiograms. Despite this, we believe that in routine daily work, it is acceptable to define the vein visible on the carotid angiogram as the BV, since it drains blood from the supratentorial area, while the vessel visible on the vertebral angiogram is the posterior mesencephalic vein, draining blood from the infratentorial area. Drawing and angiographic aspects of the basal vein are presented in Figs. 9.2, 9.3, 9.4, 9.5, 9.6, 9.7, 9.8, 9.9, and 9.10.