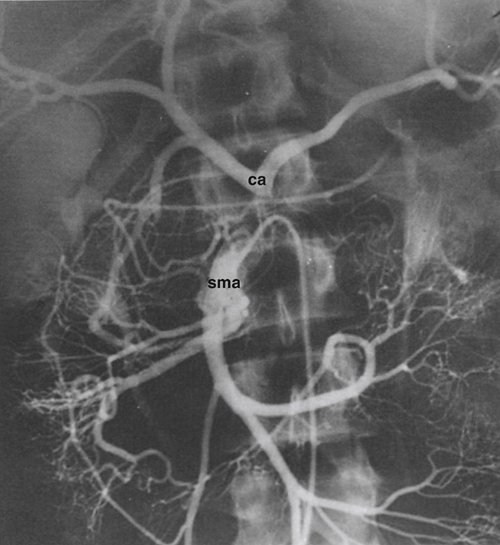
Celiac artery compression syndrome was first described in the 1960s. It is a consequence of extrinsic compression by the median arcuate ligament of the celiac artery and surrounding neural tissues (Figure 1). Several synonyms have been applied to this condition, including celiac axis syndrome, celiac band syndrome, Dunbar’s syndrome, and the median arcuate ligament syndrome. Controversy surrounds the existence of this syndrome because many asymptomatic persons have evidence of celiac artery compression, and caution is appropriate in assigning clinical relevance to the mere anatomic presence of a celiac artery narrowing. Median arcuate ligament entrapment of the celiac artery as an anatomic finding dates to 1917, long before the clinical peculiarities attending it were described in the 1960s. Minor indentations along the superior border of the celiac artery by the ligament affect approximately 40% of the adult population. In 15% of cases, more severe narrowings can result in celiac artery occlusion and the development of extensive gastroduodenal and pancreaticoduodenal collateral vessels between the superior mesenteric artery (SMA) and celiac artery circulations (Figure 2). Three factors appear to contribute to the celiac artery narrowings. First is an abnormally low-lying fibrous median arcuate ligament, which compresses and kinks a normally located celiac artery (Figure 3). Second, the celiac artery can originate higher than usual in the presence of a normally positioned median arcuate ligament. In regard to these two scenarios, both female patients and thin patients have been found to have atypically low-lying diaphragms as well as high origins of their celiac artery. Third, an excessive collection of constricting neural and fibrous tissue can entrap and narrow the celiac artery origin.
Celiac Artery Compression Syndrome

Anatomic Basis of Arterial Entrapment

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


