Cavitary Lung Disease
GENERAL PRINCIPLES
• Cavitary lung diseases may arise from a broad range of disease processes.
• Cavitation may represent an active, latent, or resolved condition.
Definition
• Pathologic definition: air-filled spaces within a nodule, mass, or area of consolidation produced by expulsion of the necrotic debris via the bronchiolar tree.
• Radiologic definition: lucent areas within the lung that may or may not contain an air–fluid level that is surrounded by a wall, usually of varied thickness.
• Other conditions such as cysts, bullae, and pneumatoceles may be incorrectly referred to as cavities.
Epidemiology
• The epidemiology of cavitary lung disease is related to the epidemiology of the underlying disease process.
• There is limited data on what the incidence of cavitation by itself is in the overall population.
Etiology
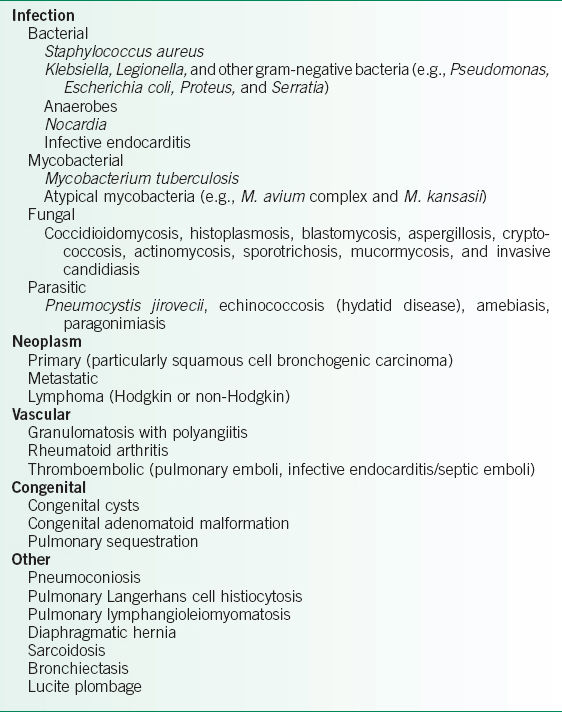
• The differential diagnosis of cavitary lung lesions is presented in Table 28-1.
• Pyogenic infections
 Necrotizing pneumonia can lead to cavitation in the setting of (or after) an acute febrile illness with productive cough.
Necrotizing pneumonia can lead to cavitation in the setting of (or after) an acute febrile illness with productive cough.
 Pyogenic abscesses develop as the ongoing infection destroys the surrounding lung parenchyma. Liquefaction necrosis and communication with the airways may develop, which leads to evacuation and expectoration of the abscess fluid, thereby producing a cavity.
Pyogenic abscesses develop as the ongoing infection destroys the surrounding lung parenchyma. Liquefaction necrosis and communication with the airways may develop, which leads to evacuation and expectoration of the abscess fluid, thereby producing a cavity.
 Causative organisms commonly include:
Causative organisms commonly include:
 Staphylococcus aureus, Klebsiella, Legionella, and other gram-negative bacteria (Pseudomonas, Escherichia coli, Proteus, and Serratia).1
Staphylococcus aureus, Klebsiella, Legionella, and other gram-negative bacteria (Pseudomonas, Escherichia coli, Proteus, and Serratia).1
 Anaerobes and mixed gram-negative organisms are more common with comorbid risk factors such as alcoholism, poor dentition, existence of otolaryngologic pathology, and aspiration pneumonia.
Anaerobes and mixed gram-negative organisms are more common with comorbid risk factors such as alcoholism, poor dentition, existence of otolaryngologic pathology, and aspiration pneumonia.
 It is rare for pneumonias caused by Mycoplasma, Chlamydia psittaci, viruses, Streptococcus pneumoniae, or Haemophilus influenzae to produce cavitary lesions, although these bacteria may still be cultured from airway secretions.
It is rare for pneumonias caused by Mycoplasma, Chlamydia psittaci, viruses, Streptococcus pneumoniae, or Haemophilus influenzae to produce cavitary lesions, although these bacteria may still be cultured from airway secretions.
 TB: cavitation is found in most cases of reactivation TB and in ∼10% of primary cases.
TB: cavitation is found in most cases of reactivation TB and in ∼10% of primary cases.
 The most common non-TB mycobacterial organisms are Mycobacterium avium-intracellulare complex and M. kansasii.
The most common non-TB mycobacterial organisms are Mycobacterium avium-intracellulare complex and M. kansasii.
• Fungal infections1
 Coccidioidomycosis: a common fungal pathogen associated with cavitary lung diseases. Endemic to the southwestern United States, Mexico, and Central and South America. Lives in the soil, and infectious airborne spores are transmitted via inhalation.3
Coccidioidomycosis: a common fungal pathogen associated with cavitary lung diseases. Endemic to the southwestern United States, Mexico, and Central and South America. Lives in the soil, and infectious airborne spores are transmitted via inhalation.3
 Histoplasmosis: found most commonly in the southeastern, mid-Atlantic, and central United States.
Histoplasmosis: found most commonly in the southeastern, mid-Atlantic, and central United States.
 Blastomycosis: seen in the Missouri and Ohio river valley states (southeastern and south central United States), the Canadian provinces bordering the Great Lakes, and the area adjacent to the St. Lawrence river in New York and Canada.
Blastomycosis: seen in the Missouri and Ohio river valley states (southeastern and south central United States), the Canadian provinces bordering the Great Lakes, and the area adjacent to the St. Lawrence river in New York and Canada.
 Aspergillus fumigatus: a ubiquitous soil fungus.
Aspergillus fumigatus: a ubiquitous soil fungus.
 Cryptococcus neoformans: usually an indolent infection found incidentally on immunocompetent patients, cavitation is typically seen in immunocompromised patients.
Cryptococcus neoformans: usually an indolent infection found incidentally on immunocompetent patients, cavitation is typically seen in immunocompromised patients.
 Actinomycosis, sporotrichosis, mucormycosis, and invasive candidiasis.
Actinomycosis, sporotrichosis, mucormycosis, and invasive candidiasis.
 Pneumocystis jirovecii (formerly Pneumocystis carinii): seen in HIV patients with CD4 count <200, transplant patients on immunosuppression, or cancer patients undergoing chemotherapy. The rate of cavitation tends to be higher in HIV-positive patients.
Pneumocystis jirovecii (formerly Pneumocystis carinii): seen in HIV patients with CD4 count <200, transplant patients on immunosuppression, or cancer patients undergoing chemotherapy. The rate of cavitation tends to be higher in HIV-positive patients.
 Parasites: hydatid cysts, amebic lung abscess, and pulmonary paragonimiasis.
Parasites: hydatid cysts, amebic lung abscess, and pulmonary paragonimiasis.
 Nocardia: a well-described cause of pulmonary infection, consolidation, and cavitation in those who are immunosuppressed or in those with alveolar proteinosis.
Nocardia: a well-described cause of pulmonary infection, consolidation, and cavitation in those who are immunosuppressed or in those with alveolar proteinosis.
• Malignancy
 Can lead to cavitation in two ways: central necrosis of the tumor itself or occludes its own blood supply, or postobstructive pneumonitis with abscess formation distal to the neoplasm.
Can lead to cavitation in two ways: central necrosis of the tumor itself or occludes its own blood supply, or postobstructive pneumonitis with abscess formation distal to the neoplasm.
 Cavitation detected by CXR is seen in 7–11% of primary bronchogenic carcinomas cavitate.1 Squamous cell carcinoma is the most common variant, cavitating >30% of the time.1,5
Cavitation detected by CXR is seen in 7–11% of primary bronchogenic carcinomas cavitate.1 Squamous cell carcinoma is the most common variant, cavitating >30% of the time.1,5
 Sarcomas cavitate more frequently than do lung carcinomas but are relatively less common.
Sarcomas cavitate more frequently than do lung carcinomas but are relatively less common.
 Both Hodgkin and non-Hodgkin lymphoma can cause pulmonary cavitation.
Both Hodgkin and non-Hodgkin lymphoma can cause pulmonary cavitation.
 Metastatic disease is often multifocal but can present as a solitary lesion as well. Few metastatic lung lesions cavitate (about 4%).1 In addition, the metastatic lesions that cavitate are most likely of squamous cell origin and can, therefore, create a diagnostic conundrum in differentiating primary versus metastatic malignancies.6
Metastatic disease is often multifocal but can present as a solitary lesion as well. Few metastatic lung lesions cavitate (about 4%).1 In addition, the metastatic lesions that cavitate are most likely of squamous cell origin and can, therefore, create a diagnostic conundrum in differentiating primary versus metastatic malignancies.6
 Keep in mind that infection can also lead to cavitary lung disease in malignant lung lesions (e.g., postobstructive pneumonia, reactivation TB from chemotherapy).1
Keep in mind that infection can also lead to cavitary lung disease in malignant lung lesions (e.g., postobstructive pneumonia, reactivation TB from chemotherapy).1
• Vascular
 Granulomatosis with polyangiitis and rheumatoid arthritis are the most common autoimmune conditions that cavitate. Perivascular inflammation within the granulomas and rheumatoid nodules leads to tissue necrosis and cavity formation in multiple locations.4
Granulomatosis with polyangiitis and rheumatoid arthritis are the most common autoimmune conditions that cavitate. Perivascular inflammation within the granulomas and rheumatoid nodules leads to tissue necrosis and cavity formation in multiple locations.4
 Cavitation occurs in up to 50% of cases of granulomatosis with polyangiitis on CT scanning, typically with a thick wall and irregular inner lining.7
Cavitation occurs in up to 50% of cases of granulomatosis with polyangiitis on CT scanning, typically with a thick wall and irregular inner lining.7
 Cavitary rheumatoid nodules are usually preceded by signs and symptoms of extrapulmonary rheumatoid disease. Caplan syndrome is the occurrence of pulmonary masses in coal miners with comorbid rheumatoid arthritis; a pneumoconiosis that is accelerated by the patient’s pre-existing autoimmune disease.
Cavitary rheumatoid nodules are usually preceded by signs and symptoms of extrapulmonary rheumatoid disease. Caplan syndrome is the occurrence of pulmonary masses in coal miners with comorbid rheumatoid arthritis; a pneumoconiosis that is accelerated by the patient’s pre-existing autoimmune disease.
 Thromboembolic disease
Thromboembolic disease
 Septic emboli: from right-sided endocarditis or infected thrombi. Lesions tend to be at the periphery of the lungs and, when cavitated, have thick walls.
Septic emboli: from right-sided endocarditis or infected thrombi. Lesions tend to be at the periphery of the lungs and, when cavitated, have thick walls.
 Pulmonary emboli (PE): rare for sterile PEs to cavitate unless there is superimposed infection.
Pulmonary emboli (PE): rare for sterile PEs to cavitate unless there is superimposed infection.
• Congenital abnormalities
 Developmental abnormalities in the primitive foregut or lung bud may produce various cystic lesions that can be mistaken as lung cavities.
Developmental abnormalities in the primitive foregut or lung bud may produce various cystic lesions that can be mistaken as lung cavities.
 Congenital adenomatoid malformation is an entity marked by multiple circumscribed radiographic lung lucencies; it is usually discovered in childhood.
Congenital adenomatoid malformation is an entity marked by multiple circumscribed radiographic lung lucencies; it is usually discovered in childhood.
 Pulmonary sequestration leads to an isolated portion of the lung possessing an independent blood supply without communication with a normal bronchus. The intralobar variant is particularly susceptible to recurrent infections and cystic or cavity formation.
Pulmonary sequestration leads to an isolated portion of the lung possessing an independent blood supply without communication with a normal bronchus. The intralobar variant is particularly susceptible to recurrent infections and cystic or cavity formation.
• Miscellaneous
 Pneumoconioses: Coal workers’ pneumoconiosis and silicosis have been associated with cavities. They produce discrete masses secondary to progressive massive fibrosis that become centrally necrotic and cavitate. Cavitation is rare, however, and its presence should always prompt one to rule out pyogenic or mycobacterial infection.
Pneumoconioses: Coal workers’ pneumoconiosis and silicosis have been associated with cavities. They produce discrete masses secondary to progressive massive fibrosis that become centrally necrotic and cavitate. Cavitation is rare, however, and its presence should always prompt one to rule out pyogenic or mycobacterial infection.
 Pulmonary Langerhans cell histiocytosis is seen in young adults, almost always associated with a significant smoking history.8
Pulmonary Langerhans cell histiocytosis is seen in young adults, almost always associated with a significant smoking history.8
 Diaphragmatic hernia may be mistaken for a cavitary lung lesion on routine CXR.
Diaphragmatic hernia may be mistaken for a cavitary lung lesion on routine CXR.
 Lucite plombage: a formerly used surgical practice of placing inert substances in the extrapleural space to induce collapse of adjacent lung for treatment of TB, produces a very characteristic appearance of multiple, tightly packed, spherical, cavitary-appearing lesions over an upper lung field.
Lucite plombage: a formerly used surgical practice of placing inert substances in the extrapleural space to induce collapse of adjacent lung for treatment of TB, produces a very characteristic appearance of multiple, tightly packed, spherical, cavitary-appearing lesions over an upper lung field.
 Other rare causes include pulmonary sarcoidosis, bronchiectasis, and amyloidosis.
Other rare causes include pulmonary sarcoidosis, bronchiectasis, and amyloidosis.
TABLE 28-1 DIFFERENTIAL DIAGNOSIS OF CAVITARY LUNG DISEASE
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


