The causes of death and heart weights at death appear to be quite different in the USA today than in the first few decades of the last century. We determined the causes of death and heart weights at necropsy in 231 adults and compared the heart weights to those reported in several studies in the first half of the 20th century. Of the 231 patients, 91 (39%) died of a cardiovascular (CV) condition, and 140 (61%), of a non-CV condition. Of the 91 fatal CV disease cases, 48 had fatal coronary artery disease (CAD); of the remaining 183 cases without fatal CAD, 25 had narrowing >75% of 1 or more major epicardial coronary arteries. Thus, 73 of the 231 (32%) patients at necropsy had severe CAD. Comparison between the fatal CV and fatal non-CV cases disclosed variable age (mean 64 years vs mean 57 years) and heart weight (529 g vs 449 g) to be significantly different. Heart weight was found to be the only significantly variable between men and women. Comparison of the heart weights in this study to those recorded as “normal” hearts 75 to 115 years earlier showed that today’s “average” heart is much larger than those reported earlier. In contrast to the earlier studies, heart weight presently appears to increase with age and with an increase in body mass index. In conclusion, early studies in heart weight did not take into account today’s longer survival and therefore a high prevalence of systemic hypertension, diabetes mellitus, obesity (and cardiac adiposity), and the presence of atherosclerotic CAD. Additionally, the cause of death (CV vs non-CV) was rarely considered in the early studies of heart weight.
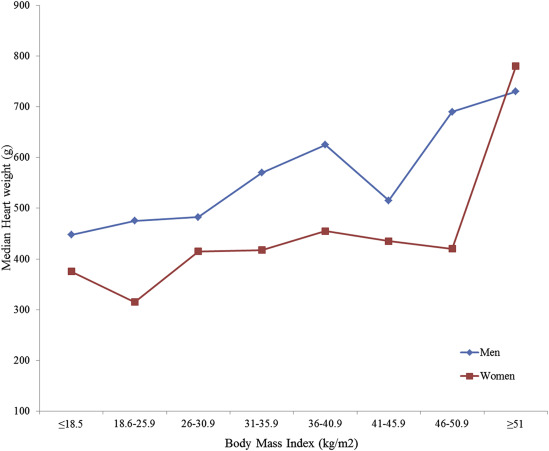
A number of publications appeared in the first half of the 20th century describing the weight of the normal and abnormal heart. A few tables appeared showing the expected normal heart weight at various ages. The problem with every one of the publications is that the heart weights were all taken from autopsy protocols, a number of different prosectors did the autopsies, and there were no standards regarding what was included in the weights. For example, was parietal pericardium totally excised before the weighting? How much of the pulmonary trunk and ascending aorta was included in the weight? How accurate were the scales? Were the scales devoid of other tissues at the time of the weighing? Additionally, adults in the first half of the 20th century were usually at or near ideal body weight compared to today when nearly 70% of the adult US population is overweight and half of them are obese. The result is a far greater quantity of adipose tissue in the heart than in earlier times. Moreover, because people in the USA today live much longer than 100 years ago (about 80 years vs about 50 years), the frequency of systemic hypertension is higher and therefore the frequency of left ventricular hypertrophy is much higher. In the present report we describe cardiac weights in 231 adults having an autopsy at Baylor University Medical Center at Dallas in 3 recent years (2013, 2014, and 2015) and in all cases the hearts were weighed by the same individual (WCR). The weights in the patients having fatal cardiovascular (CV) disease were compared to those without fatal CV disease and to previous reports on this topic. Additionally, the CV and non-CV causes of death were analyzed.
Methods
During the 3 full years of 2013, 2014, and 2015, a total of 266 autopsies were performed in adults (all >20 years of age) at Baylor University Medical Center at Dallas by Dr. Joseph M. Guileyardo: in 15, the autopsy permit did not allow examination of the heart; in 11 cases, WCR did not examine the heart, and in 9 cases, the autopsy was in individuals who previously had undergone cardiac transplantation, that is, donor heart only to examine. These 35 cases were eliminated from this study. In the remaining 231 cases, the hearts were described, opened, and weighed after “cleaning” by WCR and they form the study patients.
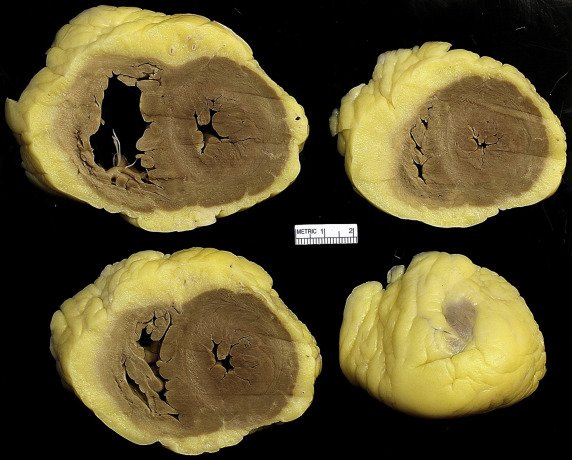
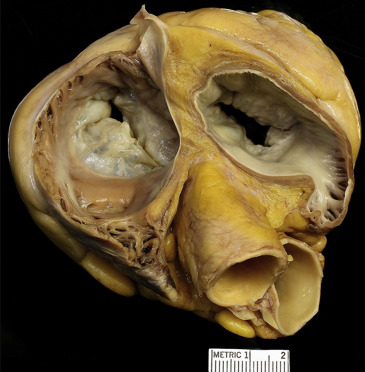
Before weighing the heart, the parietal pericardium was entirely removed from the heart, the pulmonary trunk was incised about 2 cm cephalad to the level of the pulmonic valve, the ascending aorta was incised about 2 cm cephalad to the sinotubular junction, and the heart was opened in one of the following manners ( Figures 1 to 6 ): the ventricles were cut in “bread-loaf” fashion parallel to the posterior atrioventricular sulcus, each about 1-cm in thickness and the cephalad portion of the atria were “deroofed”; the hearts were opened in both left and right parasagittal cuts, or the hearts were opened in a 4-chamber cut exposing all 4 chambers in one view. Before weighing the heart after these cuts, each surface was gently patted with paper towels to remove any extraneous formaldehyde/water. Each of the 231 hearts was weighed by WCR on one of 2 scales (Ohaus Scout Pro Scale accurate to 0.1 g or Acculab Vicon Digital Scale accurate to 1.0 g). The heart weighing was done within a week of the autopsy after fixation of the heart in formaldehyde. After describing the heart and weighing it, the medical records were reviewed in each of the 231 cases.



Statistical analyses were done using Stata 14.1. Continuous variables were presented as mean (SD) or as median (range) as applicable and categorical variables as proportions. Chi-square/Fisher’s exact tests were conducted to compare proportions, and the Student t test/Wilcoxon rank-sum test were conducted to compare continuous variables as applicable. The analyses were repeated separately for men and women.
Results
Findings in the 231 cases are summarized in Tables 1 to 8 . Table 1 presents the findings in the 91 patients who died from CV disease compared to the 140 patients who died from a non-CV condition, each group divided by gender. Of the 5 variables compared (age, body mass index [BMI], heart weight, and frequency of systemic hypertension and diabetes mellitus), only heart weight was significantly different between the 2 groups: the 91 (39%) with fatal CV disease compared to the 140 (61%) without fatal CV disease had larger heart weights (mean 580 g [men] and 455 g [women] vs 508 g [men] and 393 g [women]) than in the patients who died from a non-CV condition.
| Category of Cause of Death | Cardiovascular Death | p values | |
|---|---|---|---|
| Yes | No | ||
| Men | 54 (44%) | 68 (56%) | |
| Age (years) Range [Mean] | 33-90 [63] | 24-86 [59] | 0.057 ∗ |
| Body Mass Index (kg/m 2 ) Range [Mean] | 16-52.7 [30.2] | 15.1-72.3 [30.7] | 0.75 † |
| Heart Weight (g) Range [Mean] | 375-1020 [580] | 265-1070 [508] | 0.001 † |
| Systemic Hypertension | 38 (70%) | 41 (60%) | 0.25 |
| Diabetes Mellitus | 20 (37%) | 26 (38%) | 0.89 |
| Women | 37 (34%) | 72 (66%) | |
| Age (years) Range [Mean] | 40-87 [64] | 23-86 [55] | 0.0005 ∗ |
| Body Mass Index (kg/m 2 ) Range [Mean] | 17.4-54.8 [30.6] | 14.6-52 [31.5] | 0.55 † |
| Heart Weight (g) Range [Mean] | 208-830 [455] | 142-780 [393] | 0.003 † |
| Systemic Hypertension | 25 (68%) | 46 (64%) | 0.7 |
| Diabetes Mellitus | 11 (30%) | 23 (32%) | 0.81 |
| Total | 91 (39%) | 140 (61%) | |
| Age (years) Range [Mean] | 33-90 [64] | 23-86 [57] | 0.002 ∗ |
| Body Mass Index (kg/m 2 ) Range [Mean] | 16-54.8 [30.4] | 14.6-72.3 [31] | 0.75 † |
| Heart Weight (g) Range [Mean] | 208-1020 [529] | 142-1070 [449] | <0.001 † |
| Systemic Hypertension | 63 (69%) | 87 (62%) | 0.27 |
| Diabetes Mellitus | 31 (34%) | 49 (35%) | 0.88 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


