In order to participate in a meaningful discussion of endovascular therapies or to take part in endovascular procedures, the provider or trainee needs a fundamental understanding of equipment and techniques. This chapter is designed to prepare the reader with that basic familiarity and understanding and includes sections on catheter-based technologies and thrombolytic therapy. Additionally, this chapter provides a brief discussion of post-angiogram care and complications specific to endovascular procedures. As a starter and because the use of catheters in these cases is ubiquitous, the term catheter-based should be thought of as synonymous with endovascular procedures.
I. Basic equipment.
The exponential growth of endovascular procedures to treat vascular disease and certain patterns of vascular injury has driven the development of catheter-based technology. Competition in the industry to “build the better mousetrap” has led to a seemingly countless number of endovascular tools, some of which are interchangeable. The wide array of endovascular technologies can seem at first overwhelming. However, a basic understanding of certain core elements is all that is necessary for most basic endovascular procedures. The following section describes these core tools that that are used as part of nearly all endovascular procedures: sheaths, wires, and catheters (Table 11.1). Categories of therapeutic technologies, including balloons, stents, covered stents or stent grafts, and intravascular ultrasound are described followed by a discussion of concepts related to catheter-directed thrombolysis. Finally, a summary of post-catheterization care and complications unique to endovascular procedures is provided.
The nuances of different device brands are not discussed here, as the purpose of this chapter is to provide a broad overview of each class of equipment. Where brand names are mentioned, these may imply a frequent practice of the authors but are not intended to profess superiority of a particular device. In many cases, the obvious utility of catheter-based interventions has led to widespread usage prior to FDA approval for such applications. For example, bare metal stents were originally FDA-approved only for use in the biliary tree, and covered stents for the tracheobronchial tree. The following discussion includes some off-label use of catheter-based technology and the reader is advised to consult the individual manufacturer’s guidelines for every endovascular device prior to usage.
A. Sheaths.
The primary function of sheaths is to maintain hemostatic access to the inside of the vessel once entry has been accomplished by the modified Seldinger technique. Sheaths act as ports through which wires, catheters, and other devices can be exchanged without causing trauma to the vessel or significant blood loss. The hemostatic valve at the end of the sheath through which these devices are passed from outside of the patient to inside the blood vessel is often referred to as the diaphragm. A side port, also toward the end of the sheath, allows it to be flushed proximal to the diaphragm or transduced to measure the pressure within the vessel. Sheaths are sized based on their inner diameter with 1 Fr unit equaling 0.33 mm. This is important to keep in mind, understanding that a 5 Fr sheath has a 1.65 mm inner diameter but an outer diameter that creates a slightly larger opening in the vessel. The majority of diagnostic procedures are performed through sheaths 10-12 cm long, with longer sheaths (e.g., 45 and 90 cm) available to provide a platform for endovascular procedures at distances farther from the access site. Sheaths that are shaped with preformed curves are also available, such as the popular “crossover” sheath that has a wide U shape for optimal positioning over the aortic bifurcation into the contralateral iliac or femoral artery. Using this longer preformed sheath, arteriograms and catheter-based interventions can be performed on the leg contralateral to the femoral access site
Table 11.1. Categories of catheter-based tools
Access needles
18-gauge
21-gauge micro-puncture kit
Sheaths—4 Fr and greater
Short straight (10-12 cm and 22-25 cm lengths)
Long straight (90 cm)
Preshaped crossover sheaths (45-60 cm)
Wires— 0.014 to 0.035 inches diameter (regular and exchangelength)
The smallest sheath suitable for the task at hand should be used in order to minimize the size of the hole in the vessel and lessen the risk of access site complications. The most common sheath sizes used range from 4 Fr to 10 Fr. Very large diameter sheaths up to 25 Fr are necessary to accommodate certain devices for endovascular aneurysm repair.
B. Wires.
Catheter-based interventions are initiated with placement of a wire maneuvered into a desired location using fluoroscopic guidance. Once the wire is in the desired location, the endovascular tool needed to accomplish the next step (e.g., catheter, balloon, or stent) may be placed over a wire though the sheath, with the wire acting as a rail on which the device travels. Once a wire has been positioned to its desired location, it should not be advanced or withdrawn until the given intervention is complete. Meticulous wire control or wire management is important to avoid injury to vessels or structures beyond the desired location and critical once placed beyond a stenosis targeted for therapy. Should the wire be inadvertently pulled back proximal to such a lesion, regaining wire access can be difficult; multiple wire passes can cause adverse events such as embolization or dissection.
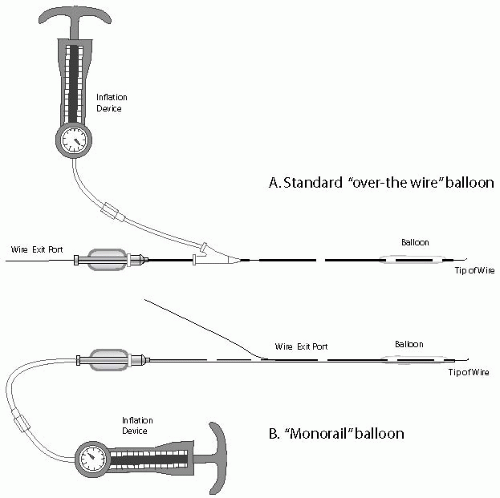
Wires are sized based on their diameters and lengths. The most common wire diameters are 0.035, 0.018, and 0.014 inches. Because they are the largest, 0.035″ wires are most easily handled and can be used for the majority of basic diagnostic and large vessel interventions. Because of their small size, 0.014-inch wires are more difficult for the less experienced endovascular specialist to handle and maneuver. The 0.014-inch wires were originally designed for use in the coronary arteries and are therefore compatible with smaller profile balloons, stents, and other endovascular devices. A benefit unique to the 0.014-inch wire pertains to monorail catheter technology. The monorail mechanism allows the wire to exit from an opening of a device (e.g., catheter, balloon, or stent) much closer to the forward tip of the device instead of out of the back or rear of the device (Fig. 11.1). This technique allows for more rapid exchanges over a shorter length of wire, reducing manipulation and making the exchange easier for one individual to accomplish. The 0.014-inch wire system is most often used in small vessels (e.g., carotids or tibials) or when wire movement must be kept to a minimum (e.g., renals). The “working wires” for the endovascular specialist include stan dard lengths (145-180 cm) and exchange lengths (240-300 cm). Exchange-length wires are necessary when performing over-the-wire interventions so that catheter or balloon exchanges can be made without losing wire access. The length of wire needed for a given procedure can be estimated using the following formula: distance from the access site to the target lesion location + length of the catheter + 10 cm.
Figure 11.1. (A) “Over-the-wire” balloons typically go over a 0.035-or 0.018-inch wire, which exits at the end of the balloon. (B) Monorail technology utilizes a 0.014-inch wire that exits via a side port in the balloon.
Wire properties also vary with respect to their steerability, trackability, and stiffness. Starter wires are used at the onset of vascular access to facilitate sheath and initial catheter placement. A typical starter wire has a low degree of stiffness and a floppy, straight, angled, or J-shaped tip that makes initial intravascular passage atraumatic. Wires with an angled tip are steerable in that the interventionalist can turn the tip in a desired direction as the wire is advanced, allowing it to navigate circuitous turns. Wires with a hydrophilic coating are useful for negotiating tortuous vessels and tight stenoses and for selecting or entering the orifice of target vessels. Hydrophilic wires are frictionless or slick when kept wet, which is a necessary step to maintain their handling and trackability. Because these wires are often too slick to manipulate with the user’s fingers alone, tools referred to as torque devices that grip the wire may be used to effectively steer or spin the tip of the wire. Care must be taken with hydrophilic wires, as they are prone to enter the subintimal plane. This can be advantageous if a subintimal angioplasty is desired, but can also create unwanted dissections or even vessel perforations. The stiffness of a wire’s body depends on its diameter and composition, although the segment at the leading edge is typically floppy.
Once the starter and hydrophilic wires have accomplished access to the desired intravascular location, an exchange to a more stiff wire is often performed to allow endovascular work over a rail with more substance. Specifically, stiff wires are often necessary to negotiate a sheath into position at a distance far from the access site without losing wire position. Stiff wires also tend to straighten tortuous vessels and provide appropriate support for the deployment of larger endovascular devices, such as endografts for aortic aneurysm repair. Examples of more stiff wires in order of increasing rigidity include the Rosen, Wholey, Meier, Amplatz, and Lunderquist wires. Finally, specially designed pressure wires are now available that can be placed to measure intravascular pressure waveforms at their distal segments or tips. These recently developed wires are useful to directly transduce intravascular pressure and to determine the presence or absence of a pressure gradient across a vascular stenosis.
C. Catheters and guiding catheters.
Catheters are long, flexible tubes with hollow lumens that are placed over and used to direct wires through vessels or across stenoses or occlusions. Once the wire has been removed from the catheter, contrast may be injected through the lumen for performance of angiography (Fig. 11.2). Catheters are sized based on their outer diameter and come in two broad categories, nonselective flush catheters and selective end-hole catheters. Nonselective angiography is performed through flush catheters, which have multiple side holes near the tip and can accommodate high pressure (400-600 psi), high flow injections without causing catheter motion (i.e., catheter whip) within the vessel during injection. Flush catheters are designed to image larger, high-flow vessels such as the aorta and vena cava and come in various lengths and shapes, including the straight flush catheter, the pigtail flush catheter and the Omni SOS catheter (AngioDynamics, Queensbury, NY, U.S.A). A wide assortment of selective or end-hole catheters is available to permit the endovascular selection or cannulation of all types of blood vessels. The choice of a particular catheter depends on the diameter and tortuosity of the main access vessel and the angle of takeoff of the branch vessel targeted for cannulation. Most often, several different catheters may be suitable for engaging a given vessel, such that the interventionalist’s preference and familiarity with the catheter is a major factor in its success. Once the catheter is engaged in the orifice of the desired vessel, the wire may be removed and a selective angiogram performed or advancement of the catheter over the wire can continue into a more distal position. Catheters with a single curve such as the angled glide, visceral selective (VS), or cobra catheters (C1-3) are advanced by simply pushing them forward over the wire. Catheters with a complex curve must be reformed within the vessel once the wire is withdrawn. Paradoxically, some complex catheters must be withdrawn by the endovascular specialist in order to allow them to advance into the vessel. Examples of complex curve catheters are the Simmons and Vitek catheters.
Figure 11.2. A sampling of commonly used catheter shapes. Catheters with a complex curve must be reformed to their preformed shape in vivo (e.g., Vitek, Simmons).
Guiding catheters, sometimes simply called guides, are essentially larger catheters through which other devices such as balloons and stents may be passed. Like catheters (and unlike sheaths), guides are measured according to their outer diameter. Therefore, an 8 Fr guide that has a 2.66 mm outer diameter will fit through an 8 Fr sheath that has the same inner diameter. The inner diameter of the guide is of course smaller and determines what size devices may pass through. Also, like catheters, guides come in a variety of preformed shapes, which facilitates their placement in angled orifices such as the renal and mesenteric arteries. Although guides can be positioned directly over a wire into a vessel’s orifice, unlike sheaths they typically do not come with a tapered inner dilator. Therefore, there is an increased risk of atheromatous embolization with this maneuver because of the stepoff (i.e., size mismatch) between the wire and the opening at the end of the guide. An alternative technique involves telescoping the guide over a catheter and wire. The catheter is then withdrawn, leaving the guide in position to conduct interventions. A Tuohy-Borst adapter may be placed over the wire and attached to the external end of the guide to prevent back-bleeding. This device allows injection of contrast through its side port into the guide to facilitate angiography while the wire remains in place, exiting out the back end of the Tuohy-Borst.
D.
Unfractionated heparin (UFH) is used during many peripheral interventions in order to prevent thrombus formation, however, consistent recommendations for its use are lacking. Higher doses of UFH (75-100 mg/kg) are often used for carotid interventions and femoral or tibial angioplasty in which the catheters or wires may be near-occlusive or when prolonged or complex interventions are anticipated. Lower doses (50 mg/kg) may be suitable for more straightforward cases such as limited iliac angioplasty. The authors also suggest lower doses of systemic heparin when working through larger femoral sheaths (7 Fr or more) or via brachial artery access. Heparin may be directly reversed with the use of protamine at the end of the procedure or simply allowed to wear off over a period of 1-2 hours prior to removal of the access sheath. Protamine binds to heparin at a ratio of 1 mg protamine: 100 U heparin, induces histamine release, and can cause hypotension and (rarely) anaphylaxis. Accordingly, 50 mg of protamine would neutralize 5,000 units of heparin; however, the time since the heparin dose should also be considered. The half-life of unfractionated heparin varies (30 minutes to 2 hours), depending on the dose.
E.
Vasodilators can be used in select cases to alleviate distal vessel spasm related to catheter or wire manipulation. Nitroglycerine can be delivered through the sheath or catheter directly into the blood vessel in increments of 50-100 mcg. The main side effect of nitroglycerin is headache related to vasodilation. When the hemodynamic significance of a mild or moderate stenosis visualized on arteriography is in question, pressures should be transduced proximal and distal to the stenosis. This can be accomplished by transducing the end of the catheter when it is proximal to the stenosis and then slowly withdrawing the catheter across the stenosis distally. A pressure wire can also be used to measure the pressure proximal and distal to the identified stenosis. A resting mean arterial pressure gradient of greater than 5 mm Hg or systolic pressure gradient greater than 10-15 mm Hg across a stenosis is considered hemodynamically significant. If there is no resting gradient identified across a moderate stenosis, intra-arterial papaverine (10-30 mg) can be administered in attempt to unmask the gradient. Papaverine causes distal vasodilation, thereby increasing the velocity across any proximal stenosis mimicking the effects of walking or exertion. A mean arterial pressure gradient of greater than 10 mm Hg or more than 15% following administration of papaverine is significant.
II.
Catheter-based therapeutic technologies can be used in cases of acute or chronic occlusive disease, aneurysms, and even in select patterns of vascular injury. Once the endovascular specialist has decided to proceed with a catheter-based intervention, the tools for that intervention need to be selected. If a diagnostic angiogram has already been performed, the basic equipment for the case can be decided upon in advance and set aside. When the intervention is done at the same sitting as the diagnostic angiogram, the interventionalist should take a few minutes to mentally plan an approach to the lesion. The plan should then be discussed with personnel in the catheterization laboratory or operating room. The staff’s understanding of the “game plan” encourages active involvement and anticipation of the methods and tools to facilitate the treatment goal.
A. Indications for angioplasty.
Since its revival in the late 1970s, angioplasty has been used successfully to dilate or recanalize arteries or grafts in every anatomic region. Catheter-based interventions generally have lower morbidity and mortality than open surgical approaches and in some cases are less expensive since the length of hospitalization is shorter. Patient recovery is excellent, with ambulation occurring on the same or following day. However, endovascular therapies are generally less durable than operative revascularization. The specific indications and options for intervention depend upon the anatomic area being treated and are discussed in detail in the chapters on specific diseases. Guidelines such as the Trans-Atlantic Inter-Society Consensus (TASC) provide recommendations for catheter-based versus surgical treatment of lower-extremity occlusive disease (see Chapter 14). For example, a short common iliac stenosis is best treated by endovascular revascularization, whereas open surgery (aortobifemoral bypass) is more fitting for diffuse aortoiliac disease. Nonetheless, the decision for or against a catheter-based intervention should be carefully considered in the context of the anatomy, patient comorbidities, and the skill set of the interventionalist. The authors also feel that success of a given intervention must be documented by improvement of both symptoms and hemodynamic measurement (ankle brachial indices, Doppler wave forms, pulse volume recordings, or transcutaneous oxygen measurements).
B.
Percutaneous transluminal angioplasty (PTA) is the most fundamental and popular technique used for treating vascular occlusive disease and generally uses polyethylene catheters that have an inflatable balloon near the tip. Balloon angioplasty represents a variation of the original transluminal arterial dilatation described by Dotter and Judkins. The Dotter technique used a relatively large 12 Fr Teflon catheter introduced over an inner 8 Fr catheter and passed through the stenosis to dilate it. No balloon was involved. Gruntzig popularized balloon catheters in the late 1970s, and their use now is common practice.
Only gold members can continue reading. Log In or Register to continue