Chapter 32 Carotid Artery Stenting
On May 6th, 2011, the U.S. Food and Drug Administration (FDA) followed up on the January 2011 recommendation of the FDA Circulatory System Device Panel1 and approved the RX Acculink carotid stent (Abbott Vascular, Santa Clara, Calif.) for use in conjunction with Abbott’s embolic protection device (EPD), the Accunet filter. The expanded label as a result of the FDA’s approval was for treatment of extracranial carotid stenosis in symptomatic and asymptomatic patients who would otherwise be considered standard risk for surgical carotid endarterectomy (CEA). This was a landmark event because for the first time, carotid stenting, at least in the United States, qualified as a standard-of-care treatment and was no longer investigational or experimental for the majority of patients with carotid artery disease. (Earlier in [2004], the FDA had approved carotid artery stenting [CAS] for high CEA risk patients). This chapter reviews historical aspects and development of CAS, discusses stenting technique in detail, and reviews clinical trial data that support current indications for this procedure.
Historical Perspective
Carotid Endarterectomy
Surgical treatment for carotid artery stenoses was introduced in the early 1950s.2 Although early observational data suggested benefit for surgery over medical therapy, large prospective randomized trials investigating the beneficial effect of CEA on stroke reduction were not initiated until the late 1980s and early 1990s. Landmark studies including the North American Symptomatic Carotid Endarterectomy Trial (NASCET),3–6 European Carotid Surgery Trial (ECST),7 Asymptomatic Carotid Atherosclerosis Study (ACAS),8 and Asymptomatic Carotid Surgery Trial (ACST)9 confirmed the benefits of surgery over best available medical treatment for reducing the risk of stroke in both symptomatic (NASCET, ECST) and asymptomatic patients (ACAS, ACST). Carotid endarterectomy surgery is comprehensively discussed in Chapter 33.
Patients included in these surgical studies were carefully selected; specifically, subjects who were considered high CEA risk were excluded from participation. Thus, octogenarians, patients with recurrent stenosis following prior ipsilateral endarterectomy, intracranial stenosis that was more severe than the surgically accessible lesion in the neck, unstable angina pectoris, recent myocardial infarction (MI), contralateral CEA, patients on long-term anticoagulation therapy, and surgically inaccessible lesions were all excluded from these trials.3,8
Endovascular Approaches to Treat Carotid Stenosis
The mission to develop safer percutaneous endovascular solutions to treat arterial stenosis was pioneered by Dotter10 and Gruntzig and Hopff11 in the 1960s and 1970s. In 1977, Klaus Mathias, an interventional radiologist, described a catheter system that could be used for performing balloon angioplasty of cervical carotid stenosis,12 and this was followed by a few case reports of successful carotid angioplasty performed in the surgical suite.13,14 In 1984, Vitek and his neuroradiology colleagues from the University of Alabama at Birmingham (UAB)15 reported angioplasty of the innominate artery aided by balloon occlusion protection of the common carotid artery (CCA). This early report represents the first percutaneous intervention performed with the benefit of distal embolic protection. During the 1980s, clinical reports of carotid angioplasty were sporadic and limited to small single-center series of patients.16 Kachel et al. summarized the results of carotid angioplasty published in the literature through 1995 and noted that 503 of the 523 (96%) procedures were technically successful. There were no deaths, major strokes occurred in 2.1%, and minor complications were in the single digits (6.3%).17 In 1985, Rabkin and Germashev began using early-generation nitinol (an alloy of nickel and titanium) stents as an endovascular prosthesis and subsequently reported their 5-year experience.18
In March 1994, Iyer, Vitek, and Roubin initiated the carotid angioplasty program at UAB under carefully scrutinized institutional protocols.19 Initial interventions were performed using stand-alone balloon angioplasty (no stents). To maximize the luminal result, a long inflation was performed using a 5-mm over-the-wire balloon; the center port of this balloon could accommodate a 0.035-inch guidewire. Once the balloon was in place, the wire was withdrawn, and oxygenated arterial blood withdrawn from the femoral artery was infused through the center port of the balloon with the help of a special pump device, permitting a long 10-minute balloon inflation. The first four patients were treated without complications. Patient #5, a woman with contralateral carotid occlusion, presented with a transient ischemic attack (TIA) related to a high-grade stenosis in the index carotid artery and underwent an uncomplicated balloon angioplasty procedure. Despite a perfectly acceptable angiographic result, approximately an hour after the procedure, there was acute closure of the angioplastied carotid artery. Although a technically successful, urgent reintervention with recanalization and stenting of the occluded vessel was performed, the patient did not recover from the major stroke related to the acute closure and subsequently expired. This case triggered the decision by the UAB group to perform elective carotid stenting—irrespective of the angiographic results of balloon angioplasty—and primary stenting became the intervention of choice for treatment of cervical carotid stenosis. The subsequent rapid adoption of this approach by interventional cardiologists in particular, and the endovascular interventional community in general, heralded the modern era of endovascular treatment for extracranial carotid bifurcation disease.19–22
Although balloon expandable stents were used in the first 100 patients, by the summer of 1995 (when the initial patients returned for their follow-up angiograms) it became clear that these stents were prone to deformation (stent crush) because of the superficial location of the carotid artery and the associated movements of the neck.23 The Alabama group were the first to report this complication, seen in approximately 15% of patients at 6-month follow-up.23 Fortunately, stent deformation was largely a cosmetic issue, with only one patient presenting with symptoms in this series. This observation, as well as the recognition that chances for regulatory approval for balloon expandable stents for treating extracranial carotid stenosis were slim, led to the rapid introduction, testing, and adoption of self-expanding stents. Stents have all but abolished acute carotid vessel closure, and in contemporary practice, primary carotid stenting is the norm. The reader should note that unlike in coronary arteries, the risk of acute stent thrombosis and instant restenosis, two major limitations of coronary stents, are nonissues when stents are deployed in the extracranial carotid location.
In 1996, Theron et al.24 reported results from his seminal work using his triple coaxial catheter that incorporated distal balloon occlusion for providing embolic protection during carotid bifurcation angioplasty. Unfortunately, this early-generation distal protection balloon could only be used with balloon angioplasty (and not with stents). By 2000, the first investigational distal balloon occlusion EPD, the Percusurge Guardwire (Medtronic, Minneapolis, Minn.) was introduced into clinical trials in the United States. This was soon followed by a number of clinical trials, all of which included a filter as the distal EPD. Unlike Theron’s distal occlusion balloon, the Percusurge balloon—as well as all such filters—can be used with both over-the-wire and monorail stent delivery systems. As increasing clinical data became available, use of distal protection devices was recognized and accepted by many (but not all25) as an integral if not mandatory part of carotid artery dilation and stenting.26–31 In our opinion, EPDs, when selected and used appropriately, improve procedure safety by significantly reducing the risk of procedure related embolic major and fatal strokes.
The multicenter Carotid and Vertebral Artery Transluminal Angioplasty Study (CAVATAS-I)9 was conducted between 1992 and 1997 in the United Kingdom during an era when stents were neither widely available nor perceived as integral. This prospective randomized trial compared outcomes of balloon angioplasty and CEA in 504 patients; only 55 patients (26%) within the group assigned to endovascular treatment received stents. Initially, stents were used only as a bailout treatment, with increased elective use toward the end of the study; distal protection devices were not used. Major event rates within 30 days after treatment did not differ significantly between endovascular treatment and surgery: disabling stroke or death (6.4% vs. 5.9%) and any major stroke lasting more than 7 days or death (10.0% vs. 9.9%). This study also demonstrated that endovascular techniques were superior to surgery when considering other risks related to the incision in the neck and use of general anesthesia. Cranial nerve injury was reported in 8.7% of surgical patients; no events occurred in patients undergoing endovascular procedures (P < 0.0001). Major groin or neck hematomas occurred less often after endovascular treatment than after surgery (1.2% vs. 6.7%, P < 0.0015). The results of this early clinical trial set the stage for investigation of carotid stenting.
Indications and Contraindications
The indications for carotid artery revascularization have been well delineated in the recent American Stroke Association/American College of Cardiology Foundation/American Heart Association (ASA/ACCF/AHA) et al. Guideline on the Management of Patients with Extracranial Carotid and Vertebral Artery Disease32 and essentially depend on symptomatic status and severity (degree) of stenosis. Hence, before an informed decision on a treatment option can be made (surgery or percutaneous intervention), it is critically important for patients and physicians to have a good understanding of the operator as well as the center’s procedural and 30-day experience and outcomes.
Symptomatic Patients
It is well accepted that revascularization should be offered to all symptomatic patients if the diameter of the ICA is reduced more than 70% as documented by noninvasive imaging, or more than 50% as documented by catheter angiography (Table 32-1). There is, however, one important caveat: the periprocedural risk of stroke or death related to the revascularization procedure (CEA or CAS) should be under 6%.32 In symptomatic patients, there is a well-established correlation between increasing stenosis severity and stroke risk. The NASCET study3 demonstrated the benefit of CEA over medical treatment for reducing the risk of future stroke in symptomatic patients with carotid stenosis between 70% and 99%. The NASCET results also showed that symptomatic patients with a lesser degree of stenosis (between 50% and 70%) benefit less. Revascularization is typically recommended in this group if there are additional unfavorable angiographic features (e.g., ulceration or other features associated with increased risk of vessel-to-vessel embolization).
Table 32-1 Modified American Heart Association Recommendations for Carotid Artery Revascularization
| Indication Level | Symptomatic Stenosis* | Asymptomatic Stenosis* |
|---|---|---|
| Proven | 70%-99% stenosis | >80% stenosis |
| Periprocedural complication risk <6% | Periprocedural complication risk <3% | |
| Life expectancy >5 years | ||
| Acceptable | 50%-69% stenosis | >60% stenosis |
| Periprocedural complication risk <3% | Periprocedural complication risk <3% | |
| Planned CABG | ||
| Unacceptable | <49% stenosis or | <60% stenosis or |
| Periprocedural complication risk >6% | Periprocedural complication risk >5% |
CABG, coronary artery bypass graft surgery.
* Lesion severity is determined according to the North American Symptomatic Carotid Endarterectomy Trial (NASCET) methodology (i.e., the ratio between lumen diameter at the point of maximal stenosis and the lumen diameter of the non tapered segment of the distal internal carotid artery).153
Modified from Brott TG, Halperin JL, Abbara S, et al: ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease: executive summary. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery, developed in collaboration with the American Academy of Neurology and Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 57:1002–1044, 2011; and Roubin GS, Iyer S, Halkin A, et al. Realizing the potential of carotid artery stenting: proposed paradigms for patient selection and procedural technique. Circulation 113:2021–2030, 2006.
An important, albeit controversial and unsettled, issue in the treatment of symptomatic patients relates to the timing of the revascularization procedure after the index symptomatic event.33–37 Risk of a recurrent neurological event after a TIA or stroke is estimated to be between 15% and 20%, and this elevated risk persists for approximately 6 months after the initial event and underlies the rationale for the 6-month threshold for defining symptomatic patients. Proponents of early intervention i.e., within a few days of the symptomatic event. Argue that the highest risk of a recurrent event is during this early period and any delay in treatment will significantly diminish its therapeutic value, since a substantial portion of these patients would have already experienced a neurological event during the waiting period. A key reason underlying the reluctance of operators to perform revascularization (CEA or CAS) soon after a stroke (less so after a TIA) is the concern that early treatment increases the risk of hemorrhagic transformation of the culprit, (nonhemorrhagic) infarct. Although the increased risk of intracranial hemorrhage following early intervention has been challenged,33 a recent retrospective analysis38 of a large national inpatient database involving more than 57 million in-hospital admissions, conducted to determine the prevalence and risk factors of intracranial hemorrhage among patients undergoing CEA (N = 215,012) and CAS (N = 13,884), arrived at a different conclusion. Symptomatic presentations represented the minority of indications for CEA (n = 10,049 [5%]), as well as CAS (n = 1251 [10%]). Intracranial hemorrhage occurred significantly more frequently after CAS than CEA in both symptomatic (4.4% vs. 0.8%; P <0.0001) and asymptomatic presentations (0.5% vs. 0.06%; P <0.0001). Multivariate regression suggested that symptomatic presentations (vs. asymptomatic) and CAS procedures (vs. CEA) were both independently predictive of six- to sevenfold increases in the frequency of postoperative intracranial hemorrhage. The observations from this retrospective population-based analysis are at variance with observations from recent large prospective randomized trials involving symptomatic and asymptomatic patients, wherein the risk of mortality and major stroke was uniformly low in both CEA and CAS arms, and the higher incidence of neurological events in the CAS arm was a result of minor strokes (ischemic rather than hemorrhagic).39–41 Pending resolution of this issue by future studies, the current approach of waiting a minimum of 3 weeks following the index event (longer for larger strokes) is likely to continue.
Asymptomatic Patients
Asymptomatic carotid disease refers to the presence of a stenosis resulting in a 60% or greater reduction of the luminal diameter of the extracranial ICA without symptoms of ipsilateral stroke, TIA, or amaurosis fugax. Treatment of patients with asymptomatic carotid artery stenosis has become extremely controversial, with two main issues fuelling this ongoing debate42–44:
1. Which asymptomatic patients (if any) are appropriate for intervention (CEA or CAS)? Current guidelines suggest that it is reasonable to refer asymptomatic patients for ICA revascularization in the setting of more than 80% stenosis and low periprocedural risk.32
2. What should be the choice of treatment? In the event revascularization is to be performed in an asymptomatic patient, should the patient be referred for CEA or CAS?
Medical treatment vs. intervention (CEA/CAS) for asymptomatic carotid disease
Despite publication of several guidelines that provide a best assessment of current research, considerable divergence of opinion regarding care of the carotid artery remains an issue among physicians worldwide.45 One reason why enthusiasm for revascularization may be low is recognition that the annualized risk of a stroke in patients with asymptomatic carotid artery disease treated with contemporary medical treatment is low and dropping (Table 32-2). This reduction in stroke risk has been attributed to the benefits of risk-factor modification, use of antihypertensive medications,46 antiplatelet agents,47 smoking cessation, and statin therapy.48,49
Table 32-2 Annualized Stroke Risk in Asymptomatic Patients with Greater Than 50% Carotid Artery Stenosis Treated with Best Medical Therapy Available During Trial Period
The guidelines respond to this concern by limiting revascularization to those asymptomatic patients in whom periprocedural risk of a stroke or death is expected to be below 3%.32 Hence, some clinicians argue that there is an urgent need for a new three-arm randomized clinical trial for asymptomatic carotid disease that includes not only CEA and CAS but also has a medical treatment arm. A critical message from the asymptomatic CEA trials was that for surgical revascularization to be beneficial in reducing future stroke risk in asymptomatic patients (Table 32-3), the periprocedural risk of revascularization should not exceed 3%. If the risk breaches the 3% threshold, the difference in stroke risk between the medically treated arm and the surgical arm will not be significant (i.e., the benefit of stroke reduction from the surgery no longer accrues to the patient). The second Carotid Revascularization Endarterectomy versus Stenting Trial (CREST II) will be a three-arm study involving asymptomatic patients, and this protocol is currently under review for funding by the National Institutes of Health (NIH).

Identifying the asymptomatic patient at high risk for developing a stroke
Much of the controversy surrounding treatment of asymptomatic carotid stenosis could be resolved if physicians had a method of reliably identifying the asymptomatic patient at high risk for a future stroke; interventional treatment could then be selectively directed at these patients. Understandably, such an approach would greatly improve the yield and cost-effectiveness of prophylactic invasive treatment with either CEA or CAS.50 Some of the metrics that have been proposed as predictors of increased risk of ipsilateral ischemic events in asymptomatic patients with carotid stenosis include higher grades of stenosis or substantial progression of carotid stenosis to a higher grade,51,52 unfavorable plaque characteristics and composition, including plaque ulceration and echolucency,53,54 or verifying the presence or absence of microemboli by using transcranial Doppler.55–58 Other clinical and radiological markers for predicting an increased risk of stroke in asymptomatic patients include occult cerebral infarction on brain imaging studies,59 contralateral carotid occlusion,60 or detection of intraplaque hemorrhage by magnetic resonance imaging (MRI).61 Nicolaides et al.62 have suggested that combining clinical risk factors, such as diabetes and smoking, with high-risk ultrasound features (e.g., echolucent plaque) may help identify the high-risk asymptomatic patient. These are listed in Table 32-4.
Table 32-4 Postulated Clinical/Investigative Features to Identify High Stroke Risk Patients with Asymptomatic Carotid Disease
| Criteria | Author(S)/Reference |
|---|---|
| Anatomical | |
| High-grade carotid stenosis with substantial progression | Bock,51 Hirt52 |
| Contralateral carotid occlusion | AbuRahma60 |
| Plaque Characteristics | |
| Plaque composition, ulceration, or echolucency | Nicolaides,53 Spence54 |
| Intraplaque hemorrhage | Altaf 61 |
| Plaque composition and clinical risk factors | Nicolaides62 |
| Imaging | |
| Microembolization | Abbott,55 Markus,56 Spence57,58 |
| Occult cerebral infarction | Norris59 |
• Contralateral carotid occlusion and a stenosis between 60% and 80% in the index carotid artery that also supplies the territory of occluded carotid artery via collaterals.
• Bilateral greater than 70% but less than 80% stenosis.
• Magnetic resonance imaging or computed tomography (CT) findings of clinically silent (asymptomatic) prior ipsilateral stroke(s).
• Patients scheduled to undergo coronary artery bypass grafting (CABG) and/or valve surgery (especially if surgery will be performed on-pump).
In the absence of an established reliable method of identifying the asymptomatic patient with carotid stenosis at high risk for developing a future neurological event, the decision to treat is predominantly based on degree of stenosis, an approach supported by the large CEA clinical trials. The threshold for treating asymptomatic carotid stenosis is 80% or greater stenosis confirmed by angiography (NASCET criteria), with corresponding elevated duplex velocities. Although standard risk-factor modification approaches should be implemented in all these patients, there is no convincing evidence to date that risk-modifying measures by themselves will reduce stroke risk in patients with severe degrees of stenosis that cannot be further improved with revascularization when the periprocedural risk is 3% or less. This nonnegotiable low tolerance for periprocedural complications constitutes what the authors have framed as the 3% Rule of Carotid Stenting.63 How to avoid breaching this rule is central to the theme of patient selection for carotid stenting. The critical all-important task of identifying the standard-risk patient for carotid stenting (not CEA) is discussed later in the chapter.
Deciding on the type of intervention, CAS or CEA, is also discussed later.
Patient Selection for Carotid Stenting
Procedure-Related Risks
Evolution in our understanding of the concept of high stent risk
To help the interventionist decide whether stenting is an appropriate treatment for a particular patient (and lesion), it is important for the operator to understand, recognize, and differentiate the standard-risk (Box 32-1) from the high-risk CAS patient. This determination, based on an individualized analysis, is the single most important element of the CAS risk stratification process and should be performed for every patient. The designation of high stent risk has evolved over time, and in retrospect was a critical component of the learning curve of the early adopters of the CAS treatment modality. Because the attributes that define high CEA risk (Box 32-2) are distinct from those that define high stent risk, a patient who is high risk for CEA does not automatically become suitable (i.e., standard risk) for CAS. The presence of high-risk features for stenting was unrecognized during the early clinical trials and the criteria for inclusion in these trials only specified “high–CEA risk patients,” thus permitting unbalanced comparisons of technique. Hence, the high event rates observed in early high–CEA risk stent registries resulted in large part from the unwitting inclusion of high stent risk patients. With the more recent exclusion of high stent risk patients, a corresponding improvement in procedural outcomes has been noted. For example, by 2005 the concept of high stent risk was better established, and in the second half of the CREST study, many of these high-risk stent patients were generally excluded (since the CREST protocol written in the late 1990s did not specifically call out high stent risk exclusions).39 The Asymptomatic Carotid Trial (ACT-I), a trial that specifically excludes high stent risk patients, is in progress (NCT00106938).
 Box 32-1 Standard Risk for Carotid Stenting: Patient and Lesion Characteristics
Box 32-1 Standard Risk for Carotid Stenting: Patient and Lesion Characteristics







Recognize Ideal Lesion and ICA Morphology for Carotid Stenting
 Angle between the ICA and ECA is <90 degrees
Angle between the ICA and ECA is <90 degrees
 Minimal vessel tortuosity (i.e., no carotid redundancy)
Minimal vessel tortuosity (i.e., no carotid redundancy)

 No ulceration or obvious filling defects
No ulceration or obvious filling defects

 Lesion located in a straight segment (as opposed to a bend) of the ICA
Lesion located in a straight segment (as opposed to a bend) of the ICA
 Artery cephalad to the stenosis is straight (minimal bends and vessel tortuosity)
Artery cephalad to the stenosis is straight (minimal bends and vessel tortuosity)

 Box 32-2 Anatomical Features and Comorbidities Associated with High Carotid Endarterectomy Risk
Box 32-2 Anatomical Features and Comorbidities Associated with High Carotid Endarterectomy Risk
Anatomical
Surgically inaccessible lesions above C-2 or below the level of the clavicle
Contralateral carotid artery occlusion
Restenosis after a previous ipsilateral CEA
Previous head/neck radiation therapy or surgery that included the area of stenosis
Ipsilateral radical neck dissection for the treatment of cancer
Spinal immobility of the neck due to cervical arthritis
Comorbidities
Chronic Obstructive pulmonary disease (COPD) with a forced expiratory volume (FEV) 1 less than 30%
Requirement for staged and scheduled coronary artery bypass graft (CABG) or valve replacement procedures more than 30 days following the stent procedure
Recent myocardial infarction more than 72 hours and less than 30 days
Two or more major diseased coronary arteries that require revascularization (70% or more)
Standard stent risk
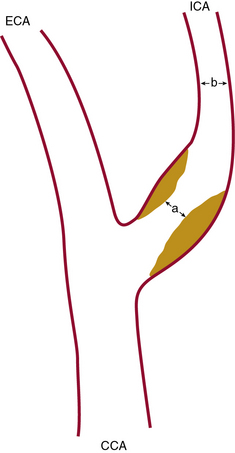
Close attention should be paid to the end-diastolic ultrasound flow velocity. If this value exceeds 100 cm/s (especially >120 cm/s), the angiographic stenosis severity will exceed 80% (as defined by the NASCET criteria; Fig. 32-1) and will meet the treatment threshold for treating asymptomatic lesions.

Figure 32-2 illustrates lesion and vessel features that are ideal for stenting using distal embolic protection. These features include:
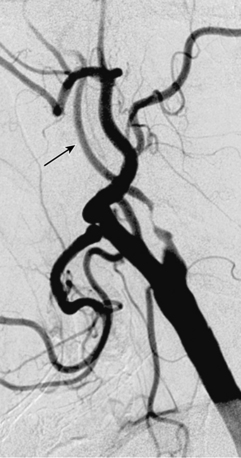
• A narrow acute angle between the ICA and external carotid artery (ECA). The wider this bifurcation (i.e., the angle approaches 90 degrees or is frankly obtuse), the greater the technical difficulty in advancing a distal embolic protection filter device with a fixed-wire system (Fig. 32-3). The technical difficulty imparted by an open ICA/ECA angle is compounded if there is additional tortuosity in the ICA distal to the stenosis (Fig. 32-4).
• Minimal calcification and no ulceration. Some degree of calcification is nearly ubiquitous in a diseased carotid bifurcation, but heavy concentric calcification in association with a severe stenosis is a major problem. Although the demonstration of carotid calcification is straightforward and requires only fluoroscopy (Fig. 32-5), the distinction between deep vessel wall calcium and superficial calcium encroaching on the vessel lumen may be difficult, and the decision to declare the case unsuitable for CAS is largely subjective. We arbitrarily define heavy calcification as calcification 3 mm or more in width, with concentricity defined by imaging in two orthogonal views. The unyielding nature of calcium, along with the stiffness it imparts to the involved vessel segment, makes it difficult to predilate and advance the EPD and stent delivery system through the lesion (especially the stent). Forcing these devices in an attempt to cross the stenosis not only increases the chances of prolapsing the sheath out of the CCA, it also increases the risk of embolization, spasm, and dissection. Inability to completely dilate and expand the deployed stent despite using larger and/or high-pressure balloons (resulting in a stent with an hourglass appearance) is an intraprocedural nightmare.
• The artery, especially cephalad to the stenosis, is free of any significant kinks or bends. Presence or absence of this key unfavorable feature is extremely important to note on preprocedure magnetic resonance angiography (MRA), computed tomographic angiography (CTA), or invasive angiography, since it increases the degree of difficulty when attempting to place a distal filter EPD. Excessive vascular tortuosity is defined as two or more bend points that are 90 degrees or greater (see Fig. 32-4). At times the tortuosity can be extreme and may impart a hairpin bend to the ICA (see Fig. 32-4). Worsening grades of tortuosity increase the difficulty when attempting to cross the stenosis and may make device delivery difficult or impossible. Straightening of the tortuous vessel segment by stiff wires or devices may result in vessel spasm and reduced antegrade flow. Thus, despite filter placement, the patient does not receive the benefit of brisk antegrade flow and may manifest ischemic symptoms in the absence of adequate collaterals. Additionally, slow flow increases the risk of fibrin deposition within the filter. The longer the dwell time of the EPD, the higher the risk of an iatrogenic thrombus. Iatrogenic tortuosity can also be introduced by placement of the sheath in a redundant carotid artery, so tortuosity should be assessed after the sheath is in place below the carotid bifurcation.
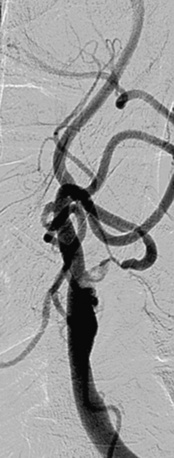

Figure 32-3 These lesions are unsuitable for carotid artery stenting using a distal embolic protection device.
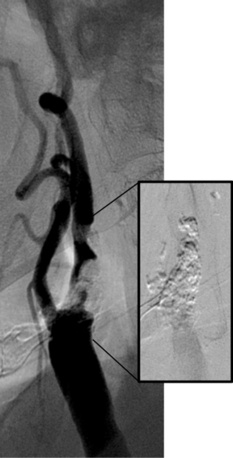
Stenosis severity and eccentricity/concentricity are not problems as long as the flow in the vessel is normal (Thrombolysis in Myocardial Infarction [TIMI] grade III). A severe stenosis in association with less than TIMI III flow (string sign, Fig. 32-6) and an occluded artery are contraindications (Fig. 32-7) for CAS. Ulceration is often noted, even on angiograms from asymptomatic patients, and although not a contraindication, operators should be aware that the risk of embolization might be higher, particularly during the phase of poststent balloon dilation. Angiographic filling defects that are consistent with a thrombus are a contraindication to CAS (Fig. 32-8). Note that both calcium and thrombus may appear as filling defects, and the differentiation is based on the clinical presentation. Whereas a filling defect in a symptomatic patient should be presumed to be thrombus (see Fig. 32-7), filling defects in asymptomatic patients are frequently a result of calcium encroaching on the vessel lumen (Fig. 32-9).


Figure 32-7 Thrombus located in proximal internal carotid artery in a patient with symptomatic carotid artery disease.
This is identified by the hazy appearance and is only visible following contrast injection.
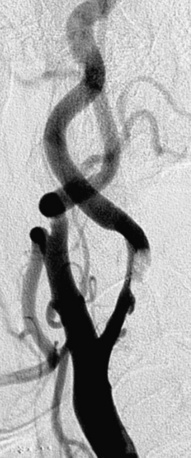
Figure 32-8 This patient demonstrates eccentric calcification, which may at times closely resemble thrombus.
Fluoroscopy without contrast injection will typically reveal calcification, as also shown in Figure 32-5.

As a rule, unfavorable anatomical features (Figs. 32-10 and 32-11; also see Figs. 32-3 through 32-9) should be considered contraindications for CAS. Although special techniques (e.g., use of a heavy-gauge buddy wire to straighten tortuous vessel segments, use of cutting balloons to dilate unyielding lesions) may result in a satisfactory angiographic outcome, the risk of a procedure-related neurological event should be presumed to breach the accepted periprocedural complication threshold.

Procedural Considerations for Carotid Artery Stenting
Initial Evaluation
Antiplatelet Agents and Anticoagulants
In the clinical protocol, great emphasis is placed on dual antiplatelet therapy before and after carotid stenting. The non-event of stent thrombosis and the low rates of peri- and postprocedural embolic events are predicated upon administration of the correct doses of adjunctive antiplatelet therapy. All patients should receive aspirin, 81 to 325 mg daily, and clopidogrel, 75 mg daily, prior to the procedure and for a minimum of 30 days after the procedure.32 If a patient has not received both aspirin and clopidogrel on a daily basis, we suggest they receive a 600-mg loading dose of clopidogrel at least 4 hours prior to the procedure. If this is not possible, the procedure should be rescheduled. There is no experience using prasugrel in patients undergoing carotid stenting.
Technique of Carotid Stenting
Technical aspects of the procedure are discussed under the following headings:
• Diagnostic Angiographic Evaluation.
• Final Angiographic Assessment.
• Embolic Protection Device and Sheath Removal and Access Site Hemostasis.
Diagnostic Angiographic Evaluation
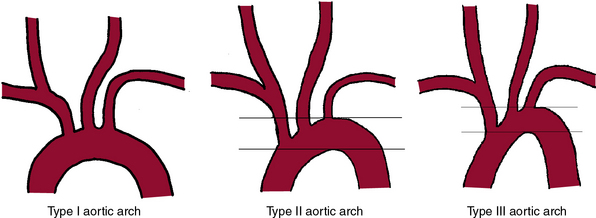
It is mandatory to have a high-quality complete diagnostic cerebral and extracranial carotid angiogram prior to initiating the stenting procedure. Imaging of the aortic arch by angiography, MRA, or CTA may be helpful to define the arch type and anomalous origins of the vessels. The most common anomaly, seen in approximately 7% of patients, is independent origin of the left vertebral artery from the arch and origin of the left carotid artery from the innominate. Figure 32-12 shows classification of the aortic arch.
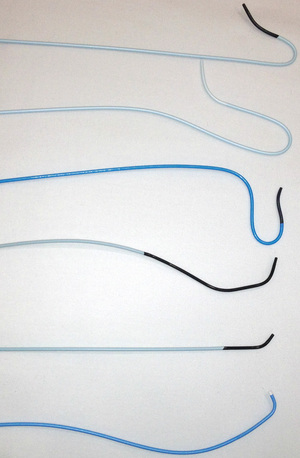
Catheter selection for diagnostic angiography
A variety of catheters are available for diagnostic cerebral angiography, and selection is tied to operator familiarity and experience. Examples of diagnostic catheters are shown in Figure 32-13. It should be understood that catheters that require additional manipulations to reshape them within the ascending aorta increase the risk of embolization. Use of such catheters should be reserved for negotiating the difficult aortic arch anatomy (e.g., patients with extended, stiff, calcified aortas [see Fig. 32-12, type III arch]) when use of alternative preshaped catheters that require less manipulation have either failed or are expected to fail.
1. It is a reliable, reproducible method for precisely measuring the degree of carotid artery stenosis (see Fig. 32-1).
2. It demonstrates anatomical conditions that can be unfavorable for carotid stenting. Examples include dilated/extended aortic arch (see Fig. 32-12), marked vessel tortuosity, heavily calcified stenosis, and lesions with obvious filling defects (see Figs. 32-3 through 32-11).
3. It helps define the status of collateral circulation to the ipsilateral cerebral hemisphere (i.e., the one supplied by the stenotic carotid artery being evaluated for treatment). Knowledge of contralateral carotid stenosis or occlusion and status of the collateral supply influences the stenting technique: shorter balloon inflations, for example, and choice of protection device—flow interrupting (occlusion balloon) vs. flow preserving (filter devices). The term isolated hemisphere describes the anatomical situation where the cerebral hemisphere of interest is entirely dependent on the ipsilateral ICA for its blood supply, owing to absence of the anterior and posterior communicating arteries.
4. It reliably demonstrates significant flow-limiting stenosis distal to the carotid bifurcation. Although the bifurcation stenosis may be treatable, the ultimate benefit of stroke reduction may not accrue to the patient because of additional cephalad disease.
5. In the event there is an intraprocedural neurological event, the postevent intracranial angiograms can be compared with the baseline preprocedure pictures.
The main risks of invasive cerebral angiography relate to the use of contrast and the possibility of a neurological event. The typical sequence of acquisition and the usual angiographic views are listed in Box 32-3.
 Box 32-3 Overview of Carotid Angiography Acquisition Views
Box 32-3 Overview of Carotid Angiography Acquisition Views
Left Subclavian Angiogram (PA View)



Selective Left Carotid Angiograms





Carotid Sheath Placement
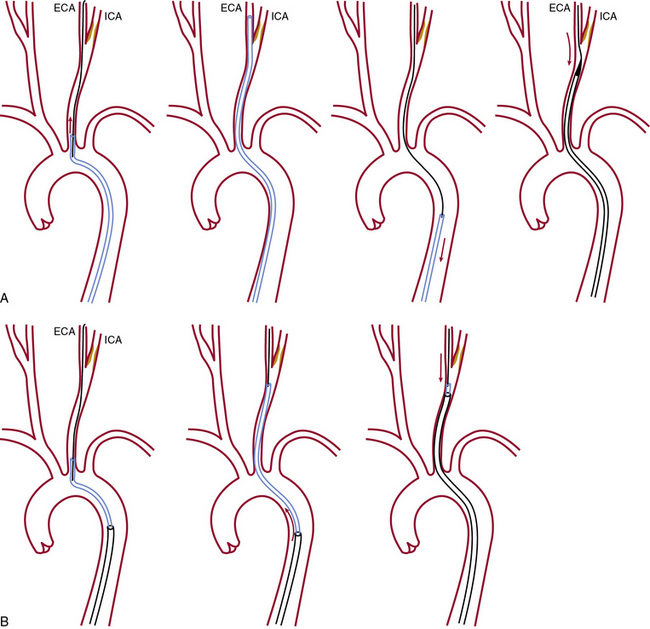
Once the diagnostic study is completed, the ICA with the target stenosis is identified, and there are no anatomical contraindications for stenting, a 90-cm long, 6 F sheath is advanced into the CCA using one of two techniques shown in Figure 32-14.
< div class='tao-gold-member'>
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


