Chapter 103
Carotid Artery
Aneurysms
Marvin D. Atkins, Ruth L. Bush
Aneurysms of the extracranial carotid arteries can occur as a result of atherosclerotic degeneration, traumatic injury, dissection, or local infection, or as a complication after carotid endarterectomy (CEA). Extracranial carotid artery aneurysm (ECAA) is an uncommon but important clinical entity. Carotid aneurysms are extremely rare in comparison with atherosclerotic occlusive disease of the same location. These aneurysms are also rare in comparison with aneurysms involving the intracranial carotid arteries and their branches. The reported incidence of incidental intracranial aneurysms discovered in autopsy studies ranges from 0.8% to 18%.1,2 The incidence of ECAA is largely unknown, but it represents only 1% to 1.5% of procedures performed for extracranial cerebrovascular disease at major referral centers.3–5 The true incidence of ECAA is well less than 1% of all carotid diseases.
Experience with endovascular carotid interventions for occlusive disease has produced technologies that have increasingly been used as minimally invasive alternatives to conventional surgical treatment of ECAAs. This chapter updates the contemporary management of ECAAs, including both open surgery and the evolving experience with endovascular therapy.
Definition
The normal carotid bifurcation is typically 40% greater in diameter than the more distal internal carotid artery (ICA). The accepted definition of most arterial aneurysms is “an artery having at least a 50% increase in diameter compared to the expected normal diameter of the artery.”6 Given this definition, it does not require much dilatation of the carotid bulb to reach this threshold, a fact that has led to disagreement about what constitutes an ECAA. deJong et al7 proposed that ECAA be defined as bulb dilatation greater than 200% of the diameter of the ICA or than 150% of the diameter of the common carotid artery. This strict definition is used in many of the contemporary reports of ECAA and is helpful, given the normal physiologic dilatation of the carotid bulb.
Historical Review
Sir Astley Cooper8 is credited with the first both unsuccessful and successful operations for ECAA in London in 1806 and 1808, respectively. Because direct surgical reconstruction was not possible, ligation of the common carotid artery was the sole treatment. Winslow9 reported an exhaustive review of 124 reported cases through 1925. In that review, 82 patients treated by carotid ligation were reported to have a mortality rate of 28%. By the 1970s, direct arterial reconstruction or autogenous vein grafting (or both) had supplanted carotid ligation. With the introduction of endovascular therapy for carotid occlusive disease, this strategy was first applied to ECAAs beginning in the 1990s.
Epidemiology
Population Affected
The population affected and age at diagnosis are directly related to the cause of the aneurysm. The relative frequency of the various potential causes of ECAA has changed over the years. Syphilis, tuberculosis, and middle ear and tonsillar infections were the most common causes of carotid artery aneurysms before the advent of antibiotics. In Winslow’s review, the majority of these early cases were pseudoaneurysms related to trauma or “erosions” from middle ear infections and tonsillitis rather than true atherosclerotic aneurysms.9 Therefore, the majority of patients were between 20 and 40 years of age, and the surgical morbidity and mortality associated with treatment were excessive. Although mycotic ECAAs were thought to be a problem of the past, a modern series reported from Durban, South Africa found 22 patients presenting with ECAAs to have human immunodeficiency virus (HIV) and/or tuberculosis, suggesting that ECAAs are more common than documented in the immunocompromised patient population.10
In modern practice, atherosclerotic degeneration, dissection, trauma, and previous carotid surgery have supplanted infection as the most frequent causes of ECAA, so the age at initial evaluation tends to mirror that of patients with carotid occlusive disease (Table 103-1).3,11–23 Increasing use of antibiotics for head and neck infections has significantly reduced the incidence of mycotic arterial infections involving the carotid artery from local extension of a septic process. ECAAs have also occurred in patients who have undergone extensive surgery and radiation therapy for head and neck cancer.24
Table 103-1
Data from the 14 Largest Single-Center Experiences with Extracranial Carotid Artery Aneurysms Since 1950*
| Total number of carotid procedures | 17,854 |
| Cases of extracranial carotid artery aneurysm (ECAA): | |
| Number | 434 |
| % of total | 2.4 |
| Indications for treatment (% of ECAA cases): | |
| Atherosclerotic origin | 42 |
| Pseudoaneurysm | 21 |
| Trauma | 16 |
| Dissection | 10 |
| Fibromuscular dysplasia | 7 |
| Infection | 2 |
| Other | 3 |
| Bilateral aneurysms | 6% of ECAA cases |
* Data from references 11 through 23.
Adapted from El-Sabrout R, et al: Extracranial carotid artery aneurysms: Texas Heart Institute experience. J Vasc Surg 31:702-712, 2000.
Blunt trauma, dissection, and penetrating injury to the neck can result in a carotid pseudoaneurysm. Such lesions are typically encountered in a younger population. False aneurysms after CEA performed for occlusive disease usually affect individuals in their sixth or seventh decades of life.
True degenerative carotid aneurysms affect men twice as often as women,14,25 and there does not seem to be a predilection for the right or left side. Most patients are older than 60 years, but true degenerative carotid artery aneurysms have been reported in children.26 There does not seem to be a specific racial distribution of true degenerative carotid aneurysms. Earlier reports suggested that the incidence of ECAAs coexisting with other aneurysmal disease ranged from 14% to 25%.9,12 Most modern series, however, have not reported similar findings. There have been several reports of ECAAs in patients with connective tissue disorders, including Ehlers-Danlos syndrome, neurofibromatosis, and the vasculitis of Behçet’s disease. It should be noted that in such patients, it is unwise to use autologous vein for arterial reconstruction because there has been late aneurysmal degeneration of the repairs using autologous vein. Synthetic conduits to replace the ECAA appear to be the best option at this point in this patient population.
Incidence/Prevalence
A 1979 report of a search of the world’s literature from 1687 to 1977 found only 853 ECAAs.4,5 Pooled data from the 13 largest single-center series from 1960 to 1995 demonstrated 392 aneurysms involving the extracranial carotid arteries. Including only series that reported CEA volume during that same period, 17,854 carotid procedures were performed, 276 of which were for ECAA, for a relative incidence of 1.54%. The largest single-center series reported, that by El-Sabrout et al3 from the Texas Heart Institute, included 67 ECAAs treated between 1960 and 1995. During the same period, 7394 peripheral aneurysm and 4991 carotid operations were performed at the same institution. This 1.31% relative incidence is mirrored in several other published series.13,27 These single-center series are from large referral centers, so the true incidence of ECAAs is probably less than 1% of all carotid disorders. Because these aneurysms are rare, it is impossible to define their true incidence or to determine whether their frequency is increasing. However, advances in vascular and soft tissue imaging have contributed to their greater recognition, especially in victims of trauma.28
Pathogenesis
Etiology
Degenerative/Atherosclerotic
Currently, degenerative (or atherosclerotic) is the most frequently reported pathology associated with ECAAs (40% to 70% of cases). These are “true aneurysms” (see Chapter 129). The histologic features are typically atherosclerotic (often termed degenerative), with disruption of the internal elastic lamina and thinning of the media. Although most true carotid aneurysms exhibit arteriosclerosis, it is considered a secondary event rather than a primary etiologic factor. Grossly, these aneurysms tend to be fusiform rather than saccular and are most commonly located at the bifurcation of the common carotid artery or the proximal ICA, where atherosclerotic plaque is common. Atherosclerotic aneurysms that do not involve the carotid bifurcation are frequently saccular and occur in patients with severe arterial hypertension. Most bilateral, nontraumatic ECAAs are of the saccular type.
Posttraumatic Causes
Penetrating Injury.
Penetrating injuries involving the extracranial carotid arteries can have two important vascular sequelae: arteriovenous fistula and false aneurysm formation. The incidence of carotid artery injury in civilian trauma series ranges from 12% to 17% of the total penetrating neck injuries. The jugular vein appears to be more frequently injured in most reports. Unlike military carotid injuries, civilian carotid injuries tend to be caused by blunt or stabbing mechanisms. Data from the Vietnam vascular registry suggest that most penetrating carotid injuries involve the common carotid artery.29 The incidence of false aneurysm development after penetrating carotid injury is not known. The vast majority of injuries require immediate surgical intervention. Delays in treatment can result in the development of a false aneurysm. What is not known, however, is the number of penetrating injuries that eventually heal without sequelae.
Iatrogenic injury to the carotid artery during attempted placement of a catheter in the internal jugular vein is another frequent cause of false aneurysm, the wall of which is composed of the surrounding fascial and soft tissue structures (see Chapter 129).
Blunt Cervical Injury and Carotid Dissection.
Blunt cervical carotid injury, though rare, can be a devastating injury. Blunt carotid injuries typically involve the distal cervical segment of the ICA at the skull base. These injuries present a unique set of challenges because they often occur in the setting of multisystem trauma, particularly head injuries, and symptoms are frequently attributed to traumatic brain injury. Unfortunately, because the vast majority of blunt cervical carotid injuries are diagnosed only after the development of symptoms from central nervous system ischemia, neurologic morbidity rates of up to 80% and associated mortality of up to 40% have been reported. Blunt injury to the carotid or vertebral vessels is diagnosed in approximately 1 in 1000 (0.1%) patients hospitalized for trauma in the United States. When asymptomatic patients are screened for blunt cerebrovascular injury, the incidence rises to 1% of all blunt trauma patients.
Blunt trauma to the cervical carotid arteries produces a spectrum of injury that includes vasospasm, intimal and medial tears, thrombosis, and partial or complete transection of the artery. Of the four main mechanisms associated with blunt cervical carotid injury, the most common involves hyperextension and rotation of the head and neck. The lateral articular processes and pedicles of the upper three cervical vertebrae project more anteriorly than C4 through C7, so the distal cervical ICA is prone to stretch injury during hyperextension. The styloid process has also been implicated in the pathophysiology of these injuries because it rotates independently with the skull on the dens, whereas the artery moves with the cervical spine.30 Other mechanisms of injury include a direct blow to the artery and compression between the mandible and vertebral body associated with severe hyperflexion. Basilar skull fractures involving the sphenoid or petrous bones can lacerate the artery from sharp fragments. In addition, intraoral trauma can directly injure the artery and lead to a traumatic pseudoaneurysm.
Blunt traumatic injuries to the carotid arteries can also lead to dissection and intramural hematoma, which can cause various degrees of luminal obstruction. Carotid dissection can occur spontaneously or as consequence of “minor trauma” such as chiropractic manipulation, shaving, sneezing, vomiting, and a host of other innocuous activities. Biffl et al31 proposed an injury grading scale to classify blunt carotid and vertebral artery injuries (Box 103-1). Injury of grade III refers to traumatic pseudoaneurysms and represents disruption of the continuity of the arterial wall with the development of a false aneurysm. A periarterial hematoma contained by the fascial planes and surrounding soft tissue structures is formed. This cavity, which contains blood and laminated thrombus, is in continuity with the arterial lumen and has the potential for embolization as well as expansion and rupture.
Fabian et al32 reported a large single-center experience with traumatic carotid artery injuries. Heparin was the only factor independently associated with improved neurologic outcome. When heparin anticoagulation is possible in a traumatized patient, it is the initial treatment of choice. In patients unable to tolerate anticoagulation, antiplatelet therapy is recommended. Endovascular treatment with a carotid stent in an attempt to tack down the intima, exclude the pseudoaneurysm from the circulation, and prevent distal embolization and rupture is gaining acceptance as the treatment of choice in patients with a persistent traumatic pseudoaneurysm. Some writers have suggested that a traumatic pseudoaneurysm present beyond a week warrants intervention.33 The management of symptomatic carotid and vertebral dissections not associated with pseudoaneurysms, but with significant luminal narrowing, remains controversial. There is a growing body of literature suggesting that in patients undergoing anticoagulation for carotid and vertebral dissection who remain symptomatic, endovascular stenting is a reasonable alternative treatment34,35 (see Chapter 102).
Postendarterectomy Aneurysms
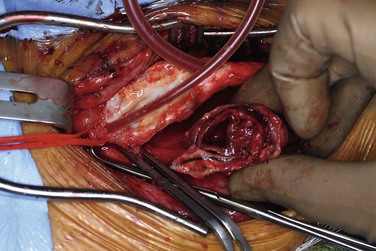
CEA-related pseudoaneurysms are some of the most frequently reported aneurysms of the extracranial carotid arteries. El-Sabrout and Cooley3 demonstrated that 57% of their 67 cases were a result of previous CEA. Zhou et al,23 in a later series from the Baylor College of Medicine, found post-CEA pseudoaneurysm to be the principal etiology in 15 (36%) of 42 cases. The development of post-CEA pseudoaneurysm is related to either suture line failure or infection. El-Sabrout and Cooley3 reported seven patients in whom the silk sutures used for patch angioplasty before the advent of monofilament sutures degenerated. Infection complicates approximately a third of all post-CEA pseudoaneurysms. The patients typically have local signs and symptoms of infection, including pain and erythema at the operative site or draining neck sinuses. Infection of the synthetic patch is identified at the time of removal, with Staphylococcus species being the most commonly cultured causative organism (Figures 103-1 and 103-2).
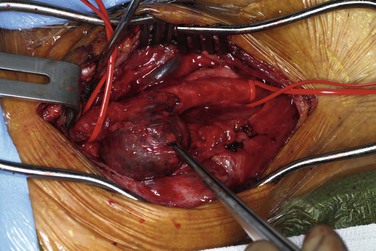
Figure 103-1 Carotid artery pseudoaneurysm (indicated by forceps) following previous endarterectomy and patch angioplasty. No infectious organisms were identified as the cause, and the patch material remained intact.
Arterial Dysplasia
Arterial dysplasia, usually a fibromuscular variant, was the most frequent pathologic cause of ECAAs reported in the series by Faggioli et al19 and also by several others.27,36 However, this finding has not been the experience documented in most other reported large series. The arteries of patients with fibromuscular dysplasia typically display a beaded appearance (alternating stenotic webs and dilatations). These dysplastic lesions may lead to ICA dissection and false aneurysm formation.
Pathology
Most primary ECAAs are secondary to a degenerative process that causes true aneurysms. Although ECAAs are frequently associated with atherosclerotic pathologic changes, the pathologic process is much more complex (see Chapter 9). There is an enormous disparity between the two types of aneurysms in the incidence of carotid occlusive disease and aneurysmal disease in the extracranial carotid artery. The rarity of primary carotid artery aneurysm in comparison with the hundreds of thousands of patients with carotid occlusive disease makes it difficult to accept atherosclerosis as the sole cause. Histologic study of carotid artery aneurysms, however, does reveal many of the findings seen in atherosclerotic specimens: fragmentation of the elastic lamina, lipid-laden foam cells, extracellular accumulation of cholesterol, deposition of hemosiderin, degeneration of the media, and neoangiogenesis. Thinning of the media and fragmentation of the internal elastic lamina are also seen, as in aging arteries. Just as many authorities propose for abdominal aortic aneurysms, atherosclerosis is a coexisting finding but may not be the primary cause.37,38
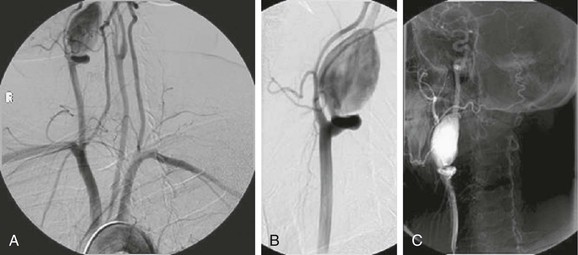
The location of aneurysms involving the extracranial carotid artery depends on the underlying pathology. True atherosclerotic aneurysms typically involve the carotid bifurcation (Fig. 103-3). Penetrating traumatic injuries usually involve the common carotid artery, and blunt traumatic injuries the distal ICA. No predisposition exists for right- or left-sided involvement in patients with unilateral aneurysms.
Clinical Findings
Physical Features/Symptoms
Pulsatile Mass
The symptoms of ECAAs vary according to their location, size, and etiology. The most common symptom is a pulsatile neck mass, which was the initial symptom in 93% of patients in the series reported by Zhou et al.23 Small internal carotid aneurysms may be asymptomatic, but most cervical carotid aneurysms are identified by the finding of a pulsating mass in the neck just below the angle of the mandible. These aneurysms may be painful, tender, or asymptomatic. Tenderness and overlying erythema, especially if associated with fever, should raise suspicion for an infected aneurysm.
ICA aneurysm is occasionally recognized as a pulsating mass in the tonsillar fossa or pharynx with little or no manifestation of its presence externally in the neck. The classic analytic study by Shipley et al39 emphasized that aneurysms of the ICA are directed inward into the throat, whereas those of the common carotid artery are directed outward into the neck. The absence of cervical swelling in the former is attributed to the dense, deep cervical fascia and muscles attached to the styloid process anteriorly and the cervical vertebrae posteriorly, which crowd the gradually dilating aneurysm inward toward the tonsillar fossa, where the thin superior pharyngeal constrictor muscle and mucous membrane offer only minimal resistance to inward protrusion. The level at which the common carotid artery bifurcates also influences the point of appearance. When the carotid bifurcation is low, an internal carotid aneurysm can be visible and palpable externally in the neck.
Aneurysms that arise at or proximal to the carotid bifurcation are readily palpable and usually pose no diagnostic difficulty. Those arising from the ICA near the base of the skull can and do cause diagnostic problems. A chronic unilateral swelling of the posterior pharynx should raise the level of suspicion, especially when other physical signs are lacking, bizarre, or atypical. Otolaryngologists are often the first to see these lesions. A high index of suspicion usually leads to computed tomography angiography (CTA), magnetic resonance angiography (MRA), or catheter-based angiography, any of which is nearly always diagnostic when an aneurysm is present.
Neurologic Symptoms
Many series report hemispheric neurologic events as the initial symptom of carotid artery aneurysms. In the Texas Heart Institute series, 28 of the 65 patients (43%) had neurologic symptoms, including amaurosis fugax and transient hemispheric ischemic attacks.3 Three of the 28 patients suffered a stroke preoperatively. Zhou et al23 reported six patients (14%) with transient ischemic attack, stroke, or Horner’s syndrome. Most neurologic events are secondary to embolization of thrombotic material from within the aneurysm wall, but some could be potentially related to diminished flow and compression of the ICA from the mass effect of large aneurysms. Transient ischemic attacks appear to occur twice as often as completed strokes.12,14,40
Cranial Nerve Dysfunction
Distal ICA aneurysms are more frequently associated with cranial nerve dysfunction than are aneurysms located more proximally, but clearly nerve injury can occur with large proximal carotid aneurysms as well. The ICA enters the cranium through the foramen lacerum and traverses the carotid canal in the petrous portion of the temporal bone. Accompanying the ICA are the sympathetic nerve fibers of the carotid plexus. Compression of these fibers can result in Horner’s syndrome, which consists of ptosis, miosis, anhidrosis, enophthalmos, and vasodilatation affecting the facial and cervical skin. Aneurysms located more proximally can result in hoarseness from compression of the vagus or recurrent laryngeal nerve. Compression of the facial nerve can cause severe facial pain. Compression of the fifth (trigeminal) and sixth (abducens) cranial nerves has been reported as well.
Dysphagia
Occasionally, the mass of a large aneurysm can cause difficulty swallowing. Protrusion of the aneurysm into the pharyngeal constrictor muscles can produce the sensation of dysphagia as well as compression of the nerves involved in the swallowing mechanism. On occasion these aneurysms are discovered during evaluation for dysphagia.
Hemorrhage and Rupture
Fortunately, hemorrhage and rupture are now infrequent manifestations of carotid artery aneurysms. There have been descriptions of “herald bleeds” or multiple smaller bleeding episodes before massive rupture. These episodes are similar to the bleeding associated with aortoenteric fistula. When these aneurysms do rupture into the oropharynx, the bleeding is profound and death is usually due to suffocation and aspiration. Mycotic aneurysms are especially susceptible to rupture and bleeding, but with the advent of antibiotics, they are exceedingly rare.
Another group of patients at risk for the so-called carotid blowout syndrome24 consist of those who have received extensive head and neck radiation therapy and those undergoing extensive surgery for head and neck cancer. Lesley et al24 reported their experience with 16 actual or impending carotid ruptures in 12 patients. Ten of these patients had undergone extensive treatment of head and neck cancer. Risk factors identified for the development of carotid blowout as a complication of treatment of head and neck cancer included thrombosis of the vasa vasorum secondary to wound infection, direct exposure and desiccation of the carotid artery, stripping of the carotid sheath, exposure of the artery to saliva, adjacent tissue necrosis, pharyngeal fistula formation, and previous irradiation.
Differential Diagnosis
The differential diagnosis for a pulsatile neck mass is extensive. The most common cause is a tortuous, kinked, or coiled carotid artery. Duplex ultrasound and occasionally CTA are required to help differentiate this finding from an ECAA (see Chapter 104). Other entities in the differential diagnosis include a prominent carotid bifurcation in a thin neck, cervical lymph nodes overlying the carotid bifurcation, carotid body tumors, glomus jugulare tumors, cervical metastatic disease, branchial cleft cysts, and cystic hygromas.
Diagnostic Evaluation
Duplex ultrasound is the initial diagnostic imaging modality of choice for the evaluation of ECAAs emanating low enough in the neck to be evaluated by this modality. Aneurysms located high in the distal ICA, such as those related to blunt cervical carotid dissection, are notoriously missed by ultrasound. Such aneurysms require further imaging with CTA or MRA. MRA has the advantage of being able to distinguish old from recent thrombus, a differentiation that is particularly helpful in cases of carotid dissection. Knowledge of the strengths and weaknesses of the imaging modalities at one’s institution should direct the next noninvasive imaging study chosen (see Chapter 98).
CTA has the benefit of visualizing the relationships of bony anatomic landmarks, which are critical in deciding whether a lesion is considered “surgically inaccessible” and requires an endovascular intervention (Fig. 103-4). MRA, when obtained in conjunction with head and brain imaging, provides indispensable information regarding the circle of Willis and collateral cerebral circulation. CTA can also provide similar intracranial imaging views, depending on the institution performing it. We have found it useful to obtain both studies at our institution to provide such complementary information.
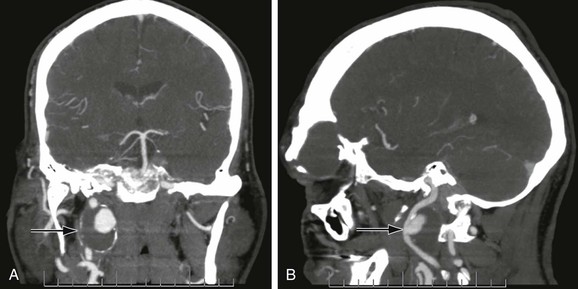
Figure 103-4 Anterior (A) and lateral (B) CT arteriogram reconstructions of a 4-cm distal internal carotid artery aneurysm (arrow). This aneurysm was treated with a covered stent graft with good result. (Courtesy Steven Oweida, MD, and John Parp Jones, MD.)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


