Cardiophrenic Angle Mass
Jud W. Gurney, MD, FACR
DIFFERENTIAL DIAGNOSIS
Common
Pericardial Cyst
Pericardial Fat Pad
Lipomatosis
Pericardial Fat Necrosis
Morgagni Hernia
Adenopathy
Less Common
Thymoma
Right Middle Lobe Collapse
Pectus Deformity
Rare but Important
Fibrous Tumor of Pleura
Impending Cardiac Volvulus
ESSENTIAL INFORMATION
Key Differential Diagnosis Issues
Mnemonic: FAT PAD
Fat
Pericardial cyst, Adenopathy, Diaphragmatic hernia
Helpful Clues for Common Diagnoses
Pericardial Cyst
Benign disorder due to anomalous outpouching of parietal pericardium
5-10% of all mediastinal masses
Location: Cardiophrenic angle
Right (70%), left (10-40%)
Size: 2-30 cm in diameter
Morphology: Round, sharp margins
Unilocular in 80%, 20% multiloculated
Wall imperceptible, noncalcified
No internal enhancement or enhancing rim
Pericardial Fat Pad
Common normal finding can mimic pneumonia on radiographs
Lipomatosis
Exuberant deposition of unencapsulated adipose tissue in mediastinum
CT: Homogeneous fat attenuation, mass does not compress or invade adjacent structures
Does not enhance with contrast
May have enlarged pericardial fat pads
Pericardial Fat Necrosis
Rare benign condition of unknown etiology
Patients usually present with acute pleuritic chest pain
Imaging and pathologic features similar to those of fat necrosis in epiploic appendagitis
Morgagni Hernia
Rare, 2% of all diaphragmatic hernias
Congenital defect through anterior parasternal hiatus between diaphragm muscle and ribs (space of Larrey)
Location: Primarily right-sided (heart limits herniation on left)
Smooth and sharply marginated
Commonly contains omental fat; may contain bowel, particularly transverse colon
Omentum contains vessels (compared to fat pads, which have sparse vessels)
Air in mass should suggest hernia
If there is pleural effusion, suspect strangulation of bowel in hernia sac
Adenopathy
Lymphadenopathy from lymphoma most common cause in this location
Metastases from tumors of thorax or abdomen may also affect these nodes
Mantle radiation therapy: Cardiac blocker used to protect heart, area undertreated
“Recurrent fat pad” sign: Enlarging recurrent nodes from lymphoma in undertreated pericardial lymph nodes
Nodes may be irradiated since field was blocked initially
Appearance or enlargement of “fat pad” heralds development of adenopathy
Helpful Clues for Less Common Diagnoses
Thymoma
Most common primary anterior mediastinal mass
Oval or lobulated mass
Homogeneous enhancement is common with small tumor, more heterogeneous enhancement for larger tumors
1/3 have calcification present on CT, usually thin and linear within capsule
Cystic regions and necrosis are common (1/3), especially with larger tumors, and may be a dominant feature
Paraneoplastic syndromes in 40%
Myasthenia gravis (35%), pure red cell aplasia (5%), hypogammaglobulinemia (10%)
Right Middle Lobe Collapse
Right middle lobe smallest of all lobes
Indirect signs from collapse uncommon; hilar shift infrequent
Lobe collapses medially toward right heart border
Right middle lobe syndrome: Cicatrizing atelectasis of RML due to prior pneumonia and poor collateral drift
RML bronchus is small, susceptible to compression from adjacent lymphadenopathy
Pectus Deformity
Pectus excavatum: 1 in 300-400 births, most common chest wall abnormality (90%)
Right heart border frequently obliterated because depressed sternum replaces aerated lung at right heart border
Heart displaced to left and rotated, may cause spurious cardiomegaly
Helpful Clues for Rare Diagnoses
Fibrous Tumor of Pleura
Uncommon primary mesenchymal tumor of pleura
80-85% benign, 15-20% malignant
Most common location: Inferior hemithorax
Often large (> 7 cm), grow very slowly over years
Lobulated, sharply marginated mass with longitudinal axis paralleling chest wall
Pedunculated lesions change location with position, a characteristic imaging feature
Rarely, pedicle may twist and detach tumor
Pleural effusion (20%), more common with malignant lesions
Calcification in 5%; calcification in malignant tumors more common (20%)
Tumors often enhance with contrast
Hypertrophic osteoarthropathy in 17-30%
Hypoglycemia rare (5%), known as Doege-Potter syndrome
Recurrence may occur even with benign tumors, requires long-term surveillance
Impending Cardiac Volvulus
Herniation of heart into hemithorax
Generally takes 3 days for adhesions to form between cut edge of pericardium and heart
Usually occurs in immediate postoperative period
Most commonly presents with sudden shock
Prior to herniation, there may be a tight, spherical, cardiac bulge (like top of snow cone) as heart begins to herniate through pericardial defect
Image Gallery
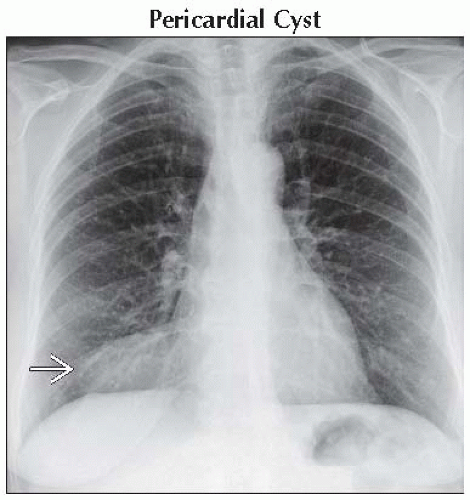 Frontal radiograph shows a mass  in the right cardiophrenic angle. The right heart border is obscured. in the right cardiophrenic angle. The right heart border is obscured. |
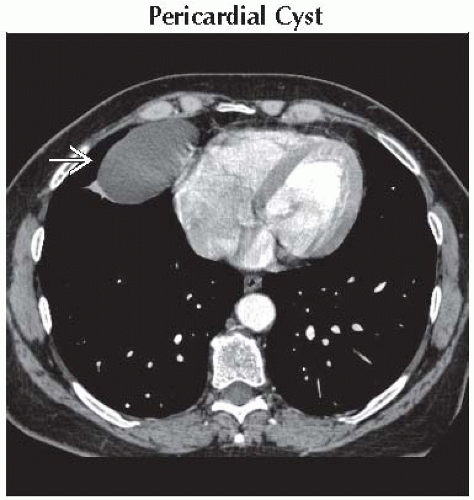 Axial CECT shows a sharply marginated, water density mass  in cardiophrenic angle. The wall of the mass is imperceptible. in cardiophrenic angle. The wall of the mass is imperceptible. |
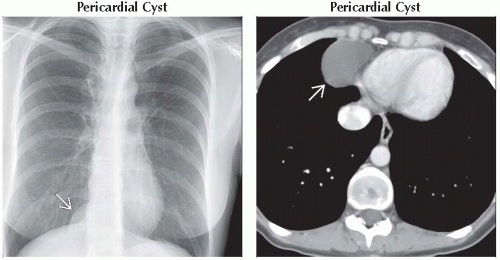 (Left) Frontal radiograph show a well-defined mass in the right cardiophrenic angle
 . (Right) Axial CECT shows a fluid-filled thin-walled cystic lesion adjacent to the right ventricle . (Right) Axial CECT shows a fluid-filled thin-walled cystic lesion adjacent to the right ventricle  with no mass effect on the heart. Cysts are typically nonseptated. Differential includes thymic cyst or bronchogenic cyst. with no mass effect on the heart. Cysts are typically nonseptated. Differential includes thymic cyst or bronchogenic cyst.Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|