ACS includes unstable angina, non-ST segment elevation MI (NSTEMI) and ST segment elevation MI (STEMI), which are each discussed in greater detail elsewhere. These subtypes of ACS represent a spectrum of the same disease process and are differentiated based on the presence of irreversible myocardial injury, as evidenced by abnormal cardiac biomarkers, and the ECG. These conditions are discussed in detail in other chapters. Briefly, most patients who present with MI are not candidates for stress testing but are typically referred directly for cardiac catheterization. STEMIs are an indication for immediate reperfusion with primary percutaneous coronary intervention or thrombolysis and NSTEMIs usually require cardiac catheterization and possibly revascularization, if appropriate.
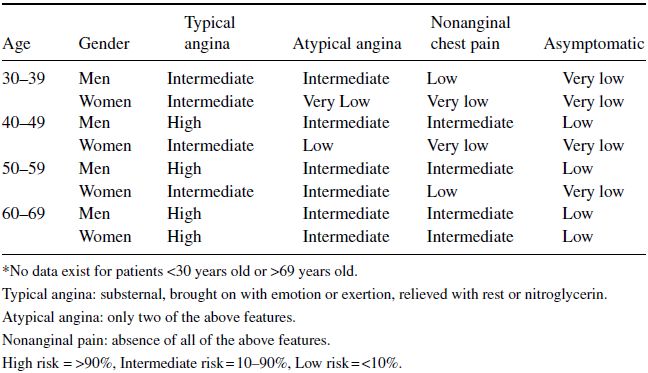
For patients who present with chest pain and no evidence of ACS, one should determine the likelihood or pre-test probability that the symptoms are due to CAD. Stress testing is most appropriate in those with an intermediate suspicion (10 to 90%) based on their pre-test probability. The assessment of pre-test probability can be based on age, gender and type of chest pain. Table 4.1 summarizes one method of determining pre-test probability of CAD; however, there are many risk stratification scores that use an array of clinical information. Bayes’ Theorem then states that the probability of a patient actually having disease is determined by multiplying their pre-test probability with the probability that the test provides a true result. This calculation is often done intuitively and influences the clinical determination of whether a test will be useful or not. For example, a 30-year-old woman with no risk factors for CAD who presents with brief, sharp non-exertional chest pain clearly has a low pretest probability for CAD, in which case a cardiac stress test would not be diagnostically valuable. Even if a stress test were positive in this patient, a false positive result is likely given the very low pretest probability of CAD.
Table 4.1 Pretest Probability of CAD by Age, Gender, and Symptoms*.
(Source: Gibbons RJ, Balady GJ, Bricker JT, et al. 2002. Reproduced with permission of Elsevier).
Cardiac stress tests are most useful as a diagnostic test in patients with an intermediate pre-test probability of CAD because the results of the test have the largest potential effect on diagnosis and future therapies. Cardiac stress tests have very limited diagnostic and prognostic value in asymptomatic, low-risk individuals. False-positive stress tests in these individuals may cause unnecessary follow-up, additional procedures, anxiety, and unwarranted exercise restriction.
4.3 POST-MYOCARDIAL INFARCTION
In contrast to its use as a diagnostic test, cardiac exercise stress testing can be useful after MI or unstable angina to determine risk and prognosis. However, the decision for exercise testing early after MI relies heavily on previous therapies and the clinical status of the patient. Cardiac exercise stress testing after MI helps with: (1) risk stratification and assessment of prognosis; (2) determining functional capacity for activity prescription after hospital discharge; and (3) assessing adequacy of medical therapy and the need to use other diagnostic or treatment options.
Sub-maximal exercise tests are preferred in patients who have not been revascularized and/or did not receive a cardiac catheterization. Sub-maximal exercise stress tests involve a predetermined endpoint such as peak heart rate of 120 bpm, 70% predicted maximum heart rate, or peak metabolic equivalent of task (MET) level of 5. Functional capacity in METs derived from the exercise test can be used to estimate tolerance for specific activities. Most domestic chores and activities require fewer than 5 METs; hence, a sub-maximal test at the time of hospital discharge can be useful in prescribing activity levels for the first several weeks after myocardial infarction.
Symptom-limited exercise tests are generally not recommended soon after myocardial infarction. If necessary, they can be ordered early after discharge (about 14–21 days) if the pre-discharge exercise test was not done or late after discharge (about 3–6 weeks) if the early exercise test was sub-maximal.
4.4 CARDIOVASCULAR STRESS TEST MODALITIES
Stress testing can be performed using electrocardiography with or without adjunctive imaging. The two major imaging modalities are echocardiography and nuclear perfusion imaging; other modalities, such as cardiovascular magnetic resonance (CMR) are much less commonly used.
Determination of which test to obtain depends on the clinical question, patient characteristics (e.g. ability to exercise, body habitus, co-morbidities), baseline electrocardiographic features, the presence of contraindications to pharmacologic agents commonly used for stress testing, and local expertise and technology (Figure 4.1).
4.5 EXERCISE STRESS TEST
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


