8 Cardiac chambers
The pitfalls that may be encountered during echocardiographic examination of the cardiac chambers relate to the diagnosis of:
PITFALLS RELATING TO CHAMBER DILATATION
Ventricular dilatation
At end-systole, the measurements are made using one of two methods:
The internal diameters of the LV are measured according to the approriate convention (Fig. 8.1, and see Fig. 7.1).
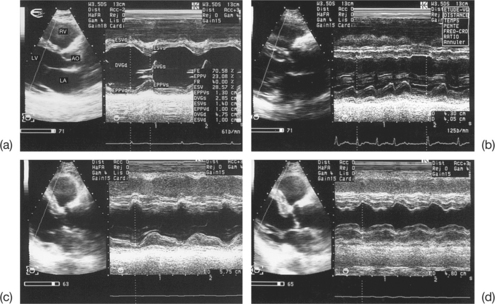
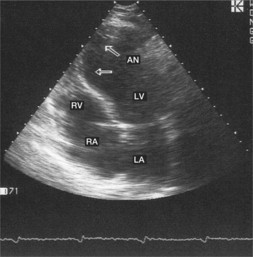
The normal values of the ventricular diameters in adults are summarized in Table 8.1. However, it is strongly recommended that the patient’s size be taken into account in order to interpret the end-diastolic diameter (EDD) of the LV, in particular. A correction of the EDD values for the body surface area is recommended. In practice, the threshold values of 56 mm (absolute values) or 32 mm/m2 (as a function of the body surface area) are more often used for EDD. Values above these thresholds confirm dilatation of the LV. However, the dilatation may be non-homogeneous, e.g. an aneurysmal dilatation involving only the apical region of the LV (Fig. 8.2). In fact, the EDD measured classically using M-mode corresponds to the internal diameter of the basal region of the LV only. A precise two-dimensional (2D) study of the size of the LV is therefore necessary in order to avoid diagnostic errors due to localized ventricular dilatations.
Table 8.1 Normal values in adults of the end-diastolic and end-systolic diameters, and the end-diastolic and end-systolic surfaces of the left ventricle (LV) in transthoracic echocardiography (TTE)
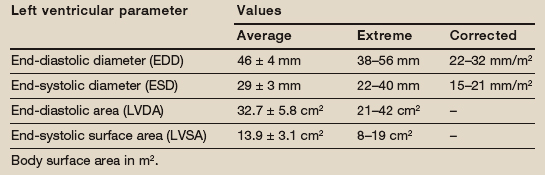
The optimum visualization of the internal contours of the LV, in the apical four-chamber projection, makes it possible to measure the left ventricular end-diastolic surface area (LVDA) and left ventricular end-systolic surface area (LVSA) using the planimetry technique (normal values are summarized in Table 8.1). However, these measures, which deliberately exclude the papillary muscles, are rarely used as a matter of routine, due to their relatively low reliability and reproducibility.
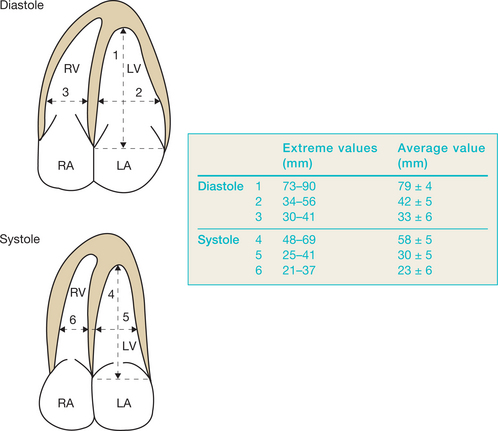
The diameters of the LV and RV may also be measured using 2D echocardiography (Fig. 8.3).
Dilatation of the atria
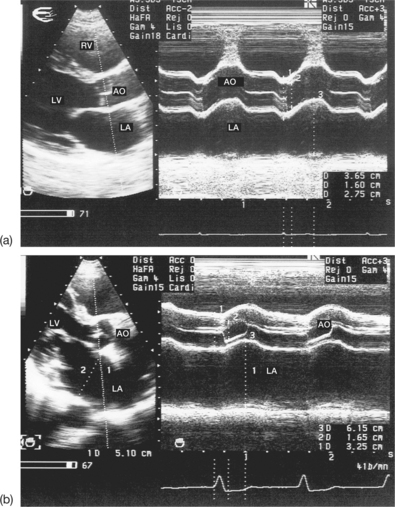
Echocardiography can be used to evaluate the diameters and the surface area of the left atrium (LA). The anteroposterior diameter of the LA is routinely measured in M-mode using the parasternal, long-axis view during end-diastole (Fig. 8.4). This is a simple measurement, and its accuracy is usually good. The potential limitations concerning the measurement of the anteroposterior diameter of the LA are:
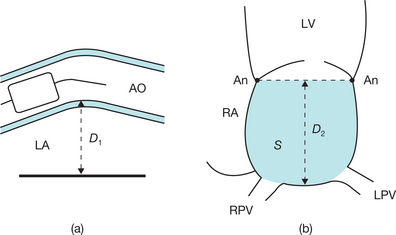
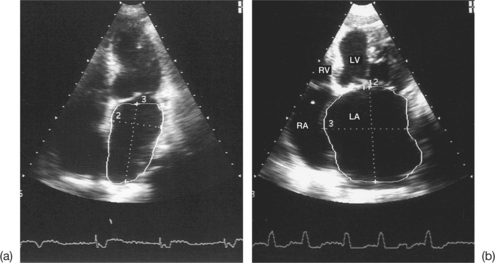
In fact, measuring only the anteroposterior diameter in the long-axis projection is insufficient in the case of asymmetrical enlargement or non-homogeneous dilatation of the LA, which is frequently observed in older patients. In these situations, it is recommended that the superoinferior diameter of the LA is also measured. This diameter is measured using the 2D mode (apical cross-section of the four chambers) from the plane of the mitral annulus to the base of the LA, during systole (Figs 8.4 and 8.6). The normal values for these two atrial diameters as measured using echocardiography are summarized in Table 8.2.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


