Figure 25.1
Thoracoscopic bulla resection. This procedure is suitable for singular bullae located peripherally on the lung surface, especially pedunculated bullae of all sizes. It is used mostly to treat primary spontaneous pneumothorax and in the concurrent management of bilateral surgery. After optimal lung collapse, thoracoscopic entry is made via two or three small ports in the lateral stretched position, exposing the bulla and its base at the lung parenchyma. At this stage, the bullae are still firm and bulging with air. A thoracoscopic inspection of the entire intrapleural cavity is necessary to assess the overall extent of the blister deformations and to determine the extent of the resection. Its objective is to resect the bulla and base from the adjacent healthy lung parenchyma to receive optimal hermetic closure of the lung surface and to avoid bleeding. To this end, endostapling devices of different lengths are used (Endo GIA; Covidien, Mansfield, MA), all with a staple cartridge at least 4.5 cm long. These devices are available commercially in various strengths (2.5, 3.5, and 4.8 mm height of the closed staples, differentiated by the colors white, blue, and green, respectively). Depending on the width of the bulla base, it might be necessary to use several cartridges for a complete resection. With pronounced emphysematous deformations and in lungs with preexisting diffuse illnesses of the parenchyma, it is advisable to buttress the Endo GIA cartridge to achieve the best pressure distribution and to avoid leakage of the parenchyma. For example, polytetrafluoroethylene sleeves that fit over the arms of surgical staplers to facilitate staple-line reinforcement may be used. With pedunculated giant bullae, sight may be impaired because of a lack of cavity space. In this case, it might be necessary to incise the wall of the bulla to enable grasping of the deflated bulla and exposing it for resection. The detached specimen may be extracted without problems by one of the minithoracotomies. The lung then is tested underwater for air leakage, which rarely occurs with parenchyma without preexisting damage, and with reinforced clamp sutures. However, these should be fixed principally by thoracoscopic sutures or by using another stapling device. Lastly, a thoracic drain is placed. Although suction usually is not essential, it might be necessary in individual cases—for example, to support reexpansion of the residual lung
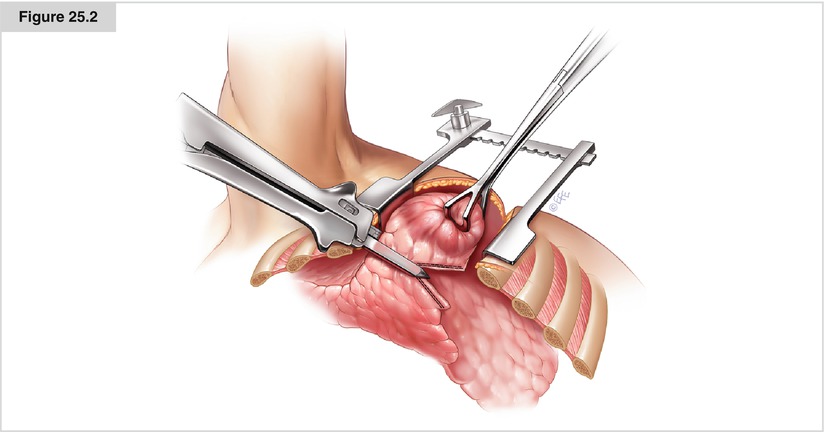
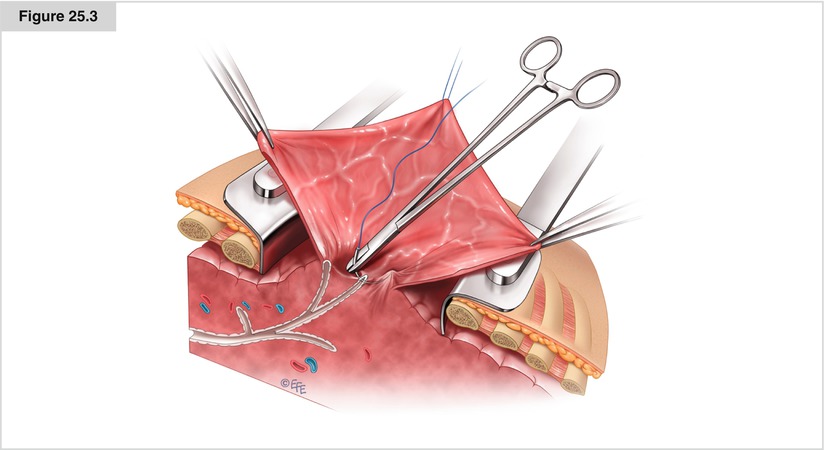
Figure 25.2
Open bulla resection by wedge resection or anatomic resection—for example, through anterolateral thoracotomy. Thoracotomy might become necessary in cases of multiple bullae of unfortunate distribution over several pulmonary lobes, sessile parenchymal bullae arising on the lung when thoracoscopy is not sufficient to control the size of lung resection, or bullae in a deep intraparenchymal location. The same applies to intralobular bullae or bullae close to the hilum. Thoracotomy also is used often for complicated bullae for which an anatomic resection might have become necessary. Usually, an anterolateral, minimally invasive (muscle-sparing) thoracotomy is sufficient. Initially, the extent of resection (wedge or anatomic resection) is determined. If an atypical resection is deemed applicable, an approach similar to that for thoracoscopic resections is used. It is necessary to resect the base of the bulla together with the nonbullous underlying lung parenchyma to obtain primary sealing of the parenchymal wound. In open surgery, Endoscopic stapling devices that fire at least double-staggered rows with up to 10-cm cartridge lengths with titanium staples also may be used. The same applies to the height of the staples. For complicated and deep intraparenchymal bullae, depending on their size, it often is necessary to carry out an anatomic wedge resection or lobectomy. In sectioning of the parenchymal bridge, the stapling devices should be buttressed if necessary. Apart from polytetrafluoroethylene sleeves, specially prepared bovine pericardial patches may be used