10 Bronchopulmonary Hygiene Therapy
Note 1: This book is written to cover every item listed as testable on the Entry Level Examination (ELE), Written Registry Examination (WRE), and Clinical Simulation Examination (CSE).
The listed code for each item is taken from the National Board for Respiratory Care’s (NBRC) Summary Content Outline for CRT (Certified Respiratory Therapist) and Written RRT (Registered Respiratory Therapist) Examinations (http://evolve.elsevier.com/Sills/resptherapist/). For example, if an item is testable on both the ELE and the WRE, it will simply be shown as: (Code: …). If an item is only testable on the ELE, it will be shown as: (ELE code: …). If an item is only testable on the WRE, it will be shown as: (WRE code: …).
MODULE A
1. Recommend starting bronchopulmonary hygiene procedures (Code: IIIG1a) [Difficulty: ELE: R, Ap; WRE: An]
2. Instruct and encourage bronchopulmonary hygiene techniques (Code: IIIC4) [Difficulty: ELE: R, Ap; WRE: An]
Teach the patient with chronic obstructive pulmonary disease the following cough techniques:
Coaching is important because patients in pain or suffering from chronic lung disease tend to be uncooperative and do not try hard. Give positive reinforcement when the patient does well. Correct any problems the patient is having following the instructions. Demonstrations are often useful so that the patient can copy a good example.
If the patient cannot cough effectively, other secretion clearance procedures will be needed. Postural drainage therapy (PDT) and other procedures follow. The American Association for Respiratory Care (AARC) Clinical Practice Guideline on PDT was used to help develop the following information. See Box 10-1 for indications for turning, postural drainage, percussion, and vibration. Contraindications are listed in Box 10-2, and recommended actions for problems are listed in Box 10-3. Beyond the patient assessment issues listed in Box 10-4, the following should be evaluated to determine whether PDT is needed:
BOX 10-1 Indications for Turning, Postural Drainage, and Percussion and Vibration
Based on information found in American Association for Respiratory Care: Clinical practice guideline: postural drainage therapy, Respir Care 36:1418, 1991.
TURNING
POSTURAL DRAINAGE
BOX 10-2 Contraindications for Turning/Postural Drainage and Percussion and Vibration
Based on information found in American Association for Respiratory Care: Clinical practice guideline: postural drainage therapy, Respir Care 36:1418, 1991.
TURNING/POSTURAL DRAINAGE*
All positions are contraindicated for patients with the following:
Trendelenburg position is contraindicated in patients with the following:
Reverse Trendelenburg position is contraindicated in patients who are:
PERCUSSION AND VIBRATION
Based on information found in American Association for Respiratory Care: Clinical practice guideline: postural drainage therapy, Respir Care 36:1418, 1991.
HAZARDS/COMPLICATIONS
BOX 10-4 Assessment of the Patient’s Needs for Postural Drainage Therapy (PDT)*
Based on information found in American Association for Respiratory Care: Clinical practice guideline: postural drainage therapy, Respir Care 36:1418, 1991.
3. Perform postural drainage (Code: IIIC1a) [Difficulty: ELE: R, Ap; WRE: An]
Postural drainage (bronchopulmonary drainage) is performed to clear secretions or prevent the accumulation of secretions. The patient is positioned so that the bronchus of a particular segment is as vertical as possible. Gravity pulls the secretions toward a major bronchus or the trachea; the secretions are then either expectorated or suctioned. The anatomy of the pulmonary lobes with their segments and respective bronchi should be reviewed (Figure 10-1).
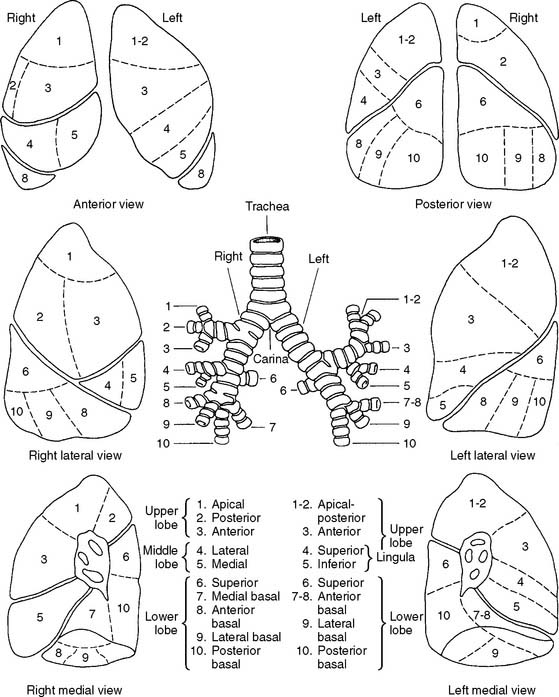
Figure 10-1 Names and locations of the lung segments and their respective bronchi.
(From Shibel EM, Moser KM, editors: Respiratory emergencies, St Louis, 1977, Mosby.)
Coughing should be encouraged after each segment is drained. The patient should not cough in a head-down position, however, because of the risk of increased intracranial pressure. Have the patient sit up to cough vigorously.
a. Pulmonary drainage positions
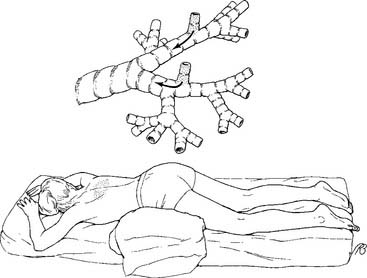
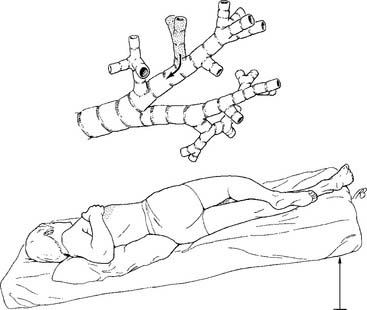
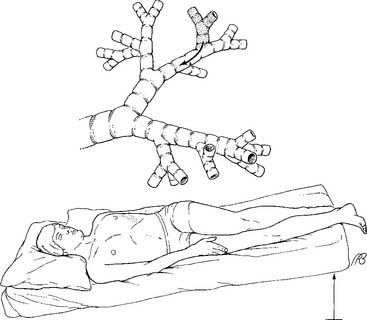
1. Lower lobes
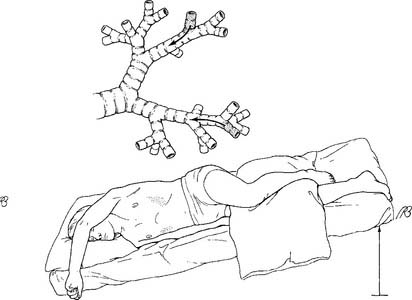
a. Posterior basal segment (Figure 10-2)
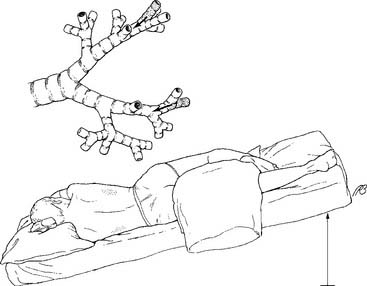
b. Lateral basal segment (Figure 10-3)
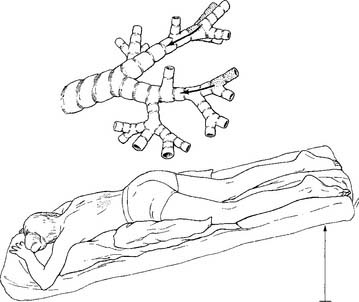
c. Anterior basal segment (Figure 10-4)
2. Right middle lobe and left lingula
a. Right lateral and medial segments (Figure 10-6)
b. Left superior and inferior lingula segments (Figure 10-7)
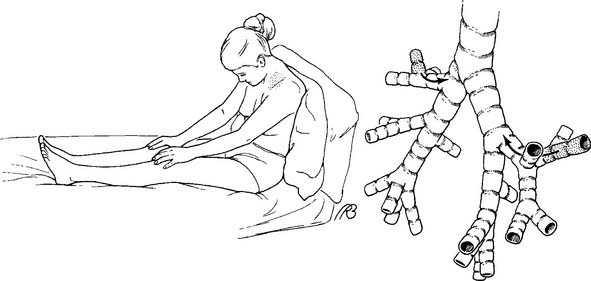
3. Upper lobes
a. Posterior segment (Figure 10-8)

b. Apical segment (Figure 10-9)
c. Anterior segment (Figure 10-10)
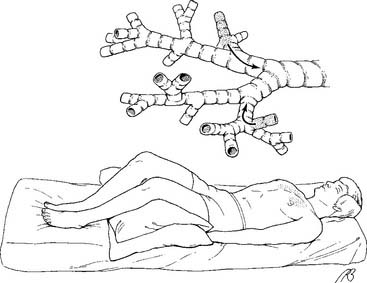
Figure 10-10 Drainage position for the anterior segments of both upper lobes.
(From Eubanks DH, Bone RC: Comprehensive respiratory care, ed 2, St Louis, 1990, Mosby.)
Some authors may list slightly different positions or several additional positions. The most commonly accepted postural drainage positions have been presented. The postural drainage positions in the infant are basically the same as those in the adult. Positioning can be accomplished more easily by using pillows. Figure 10-11 shows the various segmental drainage positions.
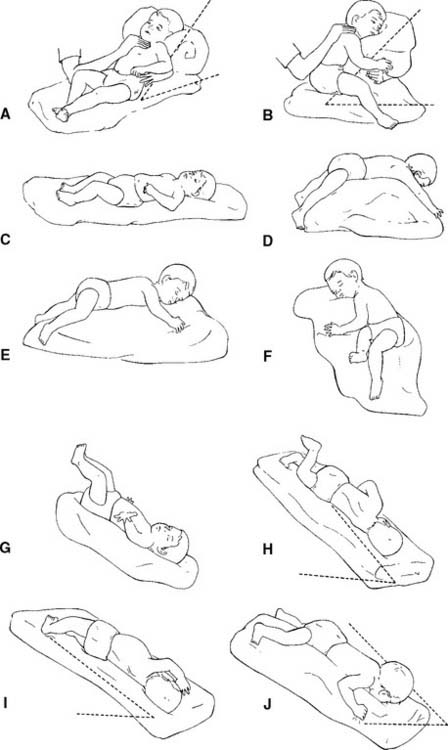
The examination usually contains at least one question that deals with knowing the correct position to drain a particular lobe. The lower lobes are usually tested. The question may give information on an opaque area seen on the chest radiograph. The therapist is expected to know what segment or lobe needs to be drained. Review Figure 1-8 for a drawing showing areas of consolidation.
4. Perform percussion (Code: IIIC1a) [Difficulty: ELE: R, Ap; WRE: An]
Percussion (also known as clapping, cupping, and tapotement) is the act of rhythmically striking the adult patient’s chest with cupped hands over an area with secretions. A properly cupped hand traps air against the chest and causes a popping sound. The wrists, elbows, and shoulders should be kept as loose as possible to enable the practitioner to keep the proper loose waving motion of the hand and minimize fatigue (Figure 10-12). Infants can be percussed by putting the index, middle, and ring fingers together into a kind of three-sided tent, or specially designed palm cups. This enables the practitioner to percuss a small area of the chest wall. Percussion is performed throughout the breathing cycle and can be done with one or both hands. Percussion should not be painful to the patient. As an added precaution, most authors recommend that the chest be covered lightly with the patient’s gown or towel. Percussion should not be done over buttons or zippers or female breast tissue.
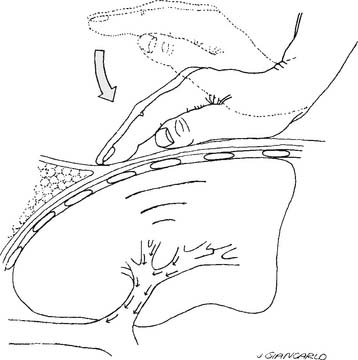
Figure 10-12 Movement of the cupped hand at the wrist during chest percussion.
(From Shapiro BA, Kacmarek RM, Cane RD, et al: Clinical application of respiratory care, ed 4, St Louis, 1991, Mosby.)
5. Perform vibration (Code: IIIC1a) [Difficulty: ELE: R, Ap; WRE: An]
Vibration is the gentle, rapid shaking of the chest wall directly over the lung segment that is being drained. It may be performed alone or with percussion. The practitioner places his or her hands side by side if the chest area is large enough or one on the other for a smaller chest area. The elbows are locked with the arms straight (Figure 10-13). The patient’s chest is gently but effectively shaken during exhalation. The patient should exhale at least the complete tidal volume (VT) as the chest wall is vibrated. Blowing out the expiratory reserve volume should help to clear out more secretions. A vibration rate of 200 per minute (about 3 per second) has been recommended as ideal to help move secretions. The literature differs as to how the patient should exhale during the procedure. Both breathing out slowly through pursed lips and breathing out forcefully through an open mouth have been recommended. A pursed-lip exhalation pattern seems reasonable if the patient has a problem with bronchospasm and air trapping. A patient without this problem should exhale forcefully because this helps to clear more secretions. Vibration should be performed for several expiratory efforts or until it is no longer effective in helping to mobilize secretions.




