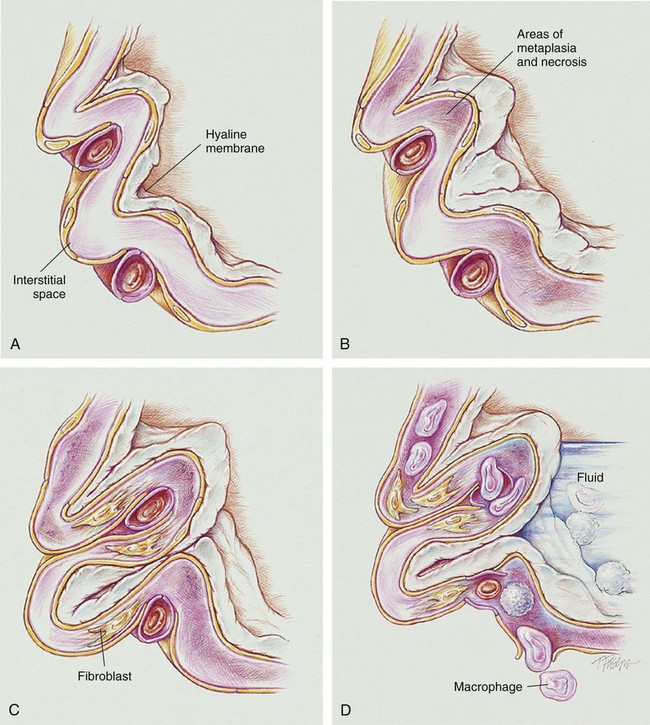
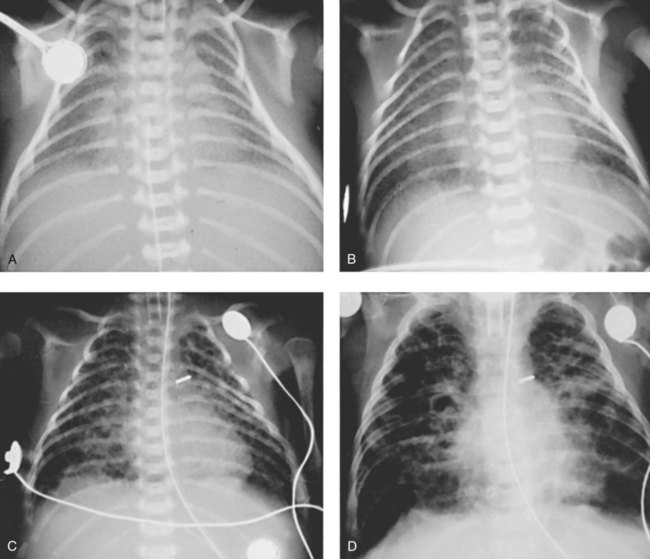
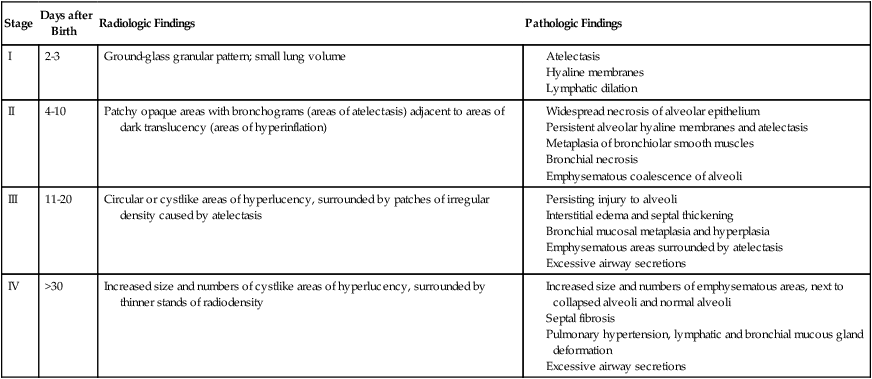
After reading this chapter, you will be able to: • List the anatomic alterations of the lungs associated with bronchopulmonary dysplasia. • Describe the causes of bronchopulmonary dysplasia. • List the cardiopulmonary clinical manifestations associated with bronchopulmonary dysplasia. • Describe the general management of bronchopulmonary dysplasia. • Describe the clinical strategies and rationales of the SOAP presented in the case study. • Define key terms and complete self-assessment questions at the end of the chapter and on Evolve. Stage I BPD was said to occur during the first 2 to 3 days of life. This stage is often indistinguishable from RDS. During this period, alveolar hyaline membranes, patches of atelectasis, and lymphatic dilation were seen. In addition, early signs of bronchial mucosal necrosis appeared during this time (see Figure 37-1, A). The chest radiographic findings revealed ground glass-like granular patterns and small lung volumes (Figure 37-2, A). Stage II BPD was said to occur 4 to 10 days after birth. Atelectasis was more extensive during this period. In addition, metaplasia of the normal lung tissue cells caused bronchial necrosis, cellular debris, partial airway obstruction, air trapping, and alveolar hyperinflation. The pathologic findings during Stage II were commonly described as alternating areas of atelectasis and of emphysema (see Figure 37-1, B). These changes appeared on chest x-ray films as patchy opaque areas with bronchograms (areas of atelectasis) next to areas of dark translucency (areas of hyperinflation) (see Figure 37-2, B). Stage III BPD was said to occur at 11 to 30 days of age. Pathologic findings included extensive bronchial and bronchiolar metaplasia and hyperplasia (an increased number of cells), interstitial fibrosis, and excessive bronchial airway secretions. In addition, the alveolar hyperinflation continued to form circular groups of emphysematous bullae that were surrounded by patches of atelectasis (see Figure 37-1, C). On the chest radiograph, the lungs began to show circular or cystic areas surrounded by patches of irregular density (see Figure 37-2, C). Stage IV BPD was said to occur after 30 days of life. During this stage, massive fibrosis of the lung and destruction of the bronchial airways, alveoli, and pulmonary capillaries occured. Areas of emphysematous, or cystlike, areas continued to increase in size and number. Thin strands of atelectasis and normal alveoli were interspersed around emphysematous areas. In addition, pulmonary hypertension often developed, lymphatic and bronchial mucous gland deformation occurred, and excessive bronchial secretions continued to be a problem (see Figure 37-1, D). The chest radiographs revealed fibrosis and edema with areas of consolidation adjacent to areas of overinflation (see Figure 37-2, D). Table 37-1 provides a summary of the original BPD stages, with pathologic and radiologic correlates. TABLE 37-1 Bronchopulmonary Dysplasia Staging (Northway) Northway WH Jr, Rosan RC, Porter DY: Pulmonary disease following respiratory therapy of hyaline-membrane disease: bronchopulmonary dysplasia, N Engl J Med 276:357-368, 1967. • Excessive bronchial secretions • Chronic alveolar fibrosis and bronchial smooth muscle hypertrophy • Bronchial mucosal metaplasia and hyperplasia • Emphysematous areas surrounded by areas of atelectasis and normal alveoli In response to the awareness of the “new” BPD, the National Institutes of Health sponsored a workshop on BPD, providing a new definition of BPD.* The new definition outlines specific diagnostic criteria, including the need for oxygen, positive pressure ventilation, and/or CPAP. The definition also includes the postnatal age to better assess the severity of BPD. Table 37-2 provides an overview of the new diagnostic criteria for the “new” BPD. TABLE 37-2 Diagnostic Criteria for the “New” Bronchopulmonary Dysplasia (BPD)
Bronchopulmonary Dysplasia
Anatomic Alterations of the Lungs
Stage
Days after Birth
Radiologic Findings
Pathologic Findings
I
2-3
Ground-glass granular pattern; small lung volume
II
4-10
Patchy opaque areas with bronchograms (areas of atelectasis) adjacent to areas of dark translucency (areas of hyperinflation)
III
11-20
Circular or cystlike areas of hyperlucency, surrounded by patches of irregular density caused by atelectasis
IV
>30
Increased size and numbers of cystlike areas of hyperlucency, surrounded by thinner stands of radiodensity
The “New” Bronchopulmonary Dysplasia—Anatomic Alterations of the Lungs
Gestational Age
<32 Weeks
≥32 weeks
Time point of assessment
36 weeks PMA or discharge to home, whichever comes first
>28 days but <56 days postnatal age or discharge to home, whichever comes first
Treatment with Oxygen >21% for at Least 28 Days, PLUS
Mild BPD
Breathing room air at 36 weeks PMA or discharge, whichever comes first
Breathing room air by 56 days postnatal age or discharge, whichever comes first
Moderate BPD
Need* for <30% oxygen at 36 weeks PMA or discharge, whichever comes first
Need* for <30% oxygen at 56 days postnatal age or discharge, whichever comes first
Severe BPD
Need* for ≥30% oxygen and/or PPV or NCPAP at 36 weeks PMA or discharge, whichever comes first
Need*
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access