Broncholithiasis
Presentation
A 52-year-old man is admitted to the pulmonary service with complaints of recurrent hemoptysis of mild to moderate severity, ongoing for the past 6 to 8 months, with occasional expectoration of blood measuring about 200 mL. The patient also reports a chronic nonproductive cough without fever, chills, weight loss, or night sweats. Past medical history includes an emergency department admission at the age of 18 years for fever, cough, dark yellowish productive sputum, and pleuritic chest pain. Since then, the patient denies a history of asthma, bronchitis, or pneumonia. He is a nonsmoking farmer who has lived in Tennessee all his life. Physical examination is remarkable only for irregular heartbeat, egophony, and whispered pectoriloquy over the right upper lung fields. His only medication is amiodarone, 200 mg daily. In the emergency department, the following chest xrays and computed tomography (CT) scans are obtained.
▪ Chest X-rays
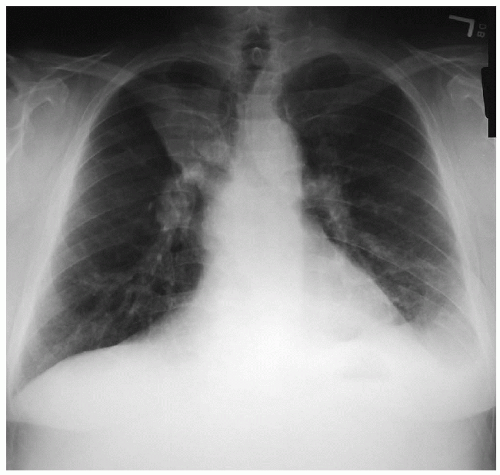 Figure 15-1 |
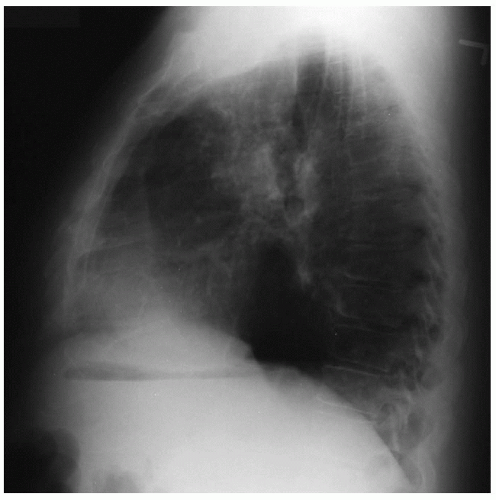 Figure 15-2 |
Chest X-ray Report
A posteroanterior and lateral chest x-ray of the chest demonstrates tracheal deviation to the right, suggesting ipsilateral volume loss. In addition, complete opacification of the right upper lobe consistent with collapse, multiple stations of calcified lymph nodes, obscured left hemidiaphragm, and costophrenic sulcus are also noted. The right heart border and the cardiophrenic angle are also not well visualized.
▪ CT Scans
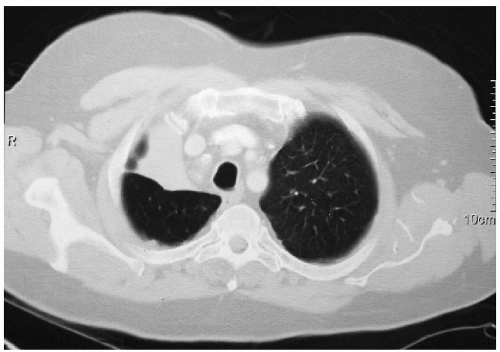 Figure 15-3 |
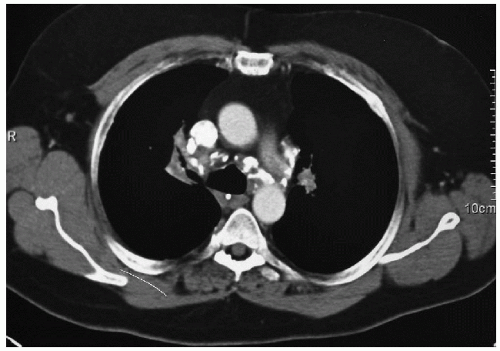 Figure 15-4 |
CT Scan Report
There is volume loss in the right upper lobe and an infiltrative pattern extending to the right hilum. The right upper lobe bronchus is encased. There are enlarged left hilar lymph nodes in addition to calcified lymph nodes at the right paratracheal, subcarinal, and aortopulmonary window regions.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


