Frequency of post-infectious bronchiolitis obliterans (PIBO)
Causes of bronchiolitis obliterans (BO)
Transplant | Graft versus host after bone marrow transplant | |
Chronic rejection after lung transplant | ||
Infections | Virus | Adenovirus: 3, 5, 7h, 21 |
Influenza | ||
Parainfluenza | ||
Measles | ||
Mycoplasma | ||
Other | Collagen disease | |
Toxic inhalation (NH3, NO2) | ||
Mineral dust | ||
Drugs | ||
Aspiration | ||
Steven–Johnson syndrome | ||
Pathology
Bronchiolitis obliterans (BO) is characterized by the partial or total occlusion of the terminal respiratory bronchiole space, caused by inflammatory tissue and fibrosis. Pathological findings in their different etiologies suggest that it would be the final process of response to different aggressions to the lower respiratory tract.
From the pathological aspect, BO may be classified in two main categories. The first one corresponds to proliferative BO, characterized by the obstruction of the space in the small airway by polyps caused by granulation tissue. If the granulation tissue extends toward the alveoli, the lesion is named BO with organizing pneumonia (BOOP). The second category is constrictive BO, which is characterized by peribronchiolar fibrosis, with different degrees of narrowing of the bronchial lumen.
Post-infectious BO is mainly characterized by a constrictive BO pattern, with different degrees of inflammation and obliteration of the airway. In these patients the signs of airway disease are frequent, such as bronchiolar inflammation, mucostasis, macrophage accumulation, and bronchiolar distortion and dilation. Bronchiolar dilations are more frequent in patients with post-infectious BO, in comparison to other causes. Histological analysis is limited by the multifocal nature of the disease.
Etiology
Different respiratory viruses, such as influenza, parainfluenza, respiratory syncytial virus (RSV), and especially adenovirus, have been associated with BO. Other infectious etiologies include Mycoplasma pneumoniae, measles virus, and human immunodeficiency virus-1. Also, in lung transplant patients, infection caused by cytomegalovirus was associated with the development of BO bronchiolitis.
In 2006 a case-control study conducted in Buenos Aires was published that included 109 patients with bronchiolitis who developed BO and 99 control patients, patients with bronchiolitis who did not progress to BO. Risk factors for developing BO were adenovirus infection (OR 49) and the need for mechanical ventilatory assistance (OR 11). Although mechanical ventilatory assistance was an independent risk factor, the results did not identify if ventilatory support was by itself the cause of the injury or if it was only an indicator of the seriousness of the disease. The main role of the infection caused by adenovirus in the development of BO was widely documented. In our study, 72% of the patients who developed BO presented with adenovirus infection. In 1984 a new adenovirus genotype, 7h, was described as one of the most virulent types, but other adenovirus such as serotypes 3, 5, and 21 can also cause BO.
Adenovirus 7h is responsible for 20% of all the infections caused by this agent, according to publications issued by the World Health Organization (WHO). In the Southern Hemisphere the incidence of the B subgene adenovirus and serotypes 4 and 7 is greater. Epidemiological studies between 1991 and 1994 in children hospitalized for lower acute respiratory infection in Argentina, Chile, and Uruguay identified that 71% of the infections caused by adenovirus where of the B subgene, and 61.2% of them corresponded to the 7h genome.
Other studies have shown that the global prevalence of adenovirus genotypes changes in relationship to time and geographic region, which makes it difficult to develop a vaccine with global effectiveness. In Argentina, during the past decade, a reduction of serious and fatal cases caused by this virus has been observed, which could be explained by a reduction of genotype 7 incidence, besides an increase of genotype 3. A reduction of infections caused by adenovirus has also been observed since 2004, perhaps because of an interference of infections caused by rhinovirus or the A H1N1 influenza pandemic in 2009.
- 1.
Epidemics during the winter months among hospitalized infants (generally under 2 years old), which cause a high rate of serious infections and death.
- 2.
Nonseasonal periodic epidemic outbreaks, community-driven, which compromise older children and adults, but cause few and infrequent respiratory sequelae.
- 3.
Epidemic outbreaks of acute respiratory diseases among military recruits.
Patients with a serious infection caused by adenovirus present with immune complex in the lung containing adenovirus antigens, as well as high levels of interleukin (IL)-6, IL-8, and tumor necrosis factor (TNF)-α serum.
Susceptibility to developing BO seems to be related to the geographic origin of human groups. The populations of native children in New Zealand, Canada, Alaska, and South America have a greater incidence of post-infectious BO when compared to the populations of Europe and other regions of America. Recent studies conducted in Argentina in patients with this disease show that the HLA haplotype DR8-DQB1∗0302, and native aborigines, determined by the mtDNA markers, are increased in relationship to control groups.
Although the studies are limited, the innate immunological response would have a preponderant role in the seriousness of the adenovirus infection and the development of BO in predisposed populations.
Infection caused by Mycoplasma pneumoniae is a frequent cause of atypical pneumonia in older children. It was identified as an etiology of BO in 1986, although its development in patients with Mycoplasma infections is a rare complication. In other areas, such as Malaysia and Korea, it is the second most common etiological agent for BO, after adenovirus infection. In these countries, infection by Mycoplasma was present in 20% of the patients with BO, most of these secondary to Mycoplasma epidemic outbreaks.
Up to 20% of influenza patients develop complications, particularly small children (0–4 years old). In spite of this, BO is a rare complication of influenza infection, and few cases in infants and small children have been published.
BO is an infrequent complication of measles. Viral load and the initial immunological condition, as well as the virus persistence in the lung parenchyma, probably determine chronic lung damage.
This virus circulation has an epidemic pattern during winter months, and it is the most common cause of lower respiratory tract infection. Association between BO and respiratory syncytial virus is rare and it is not clearly defined. Simultaneous infection of syncytial virus and adenovirus can happen. In these cases, it seems more likely that the development of BO is caused by the adenovirus infection.
Clinical Findings
In most cases, the disease starts very early, before the first year of life. However, age has not been confirmed as a risk factor for developing post-infectious BO.
Initially patients start showing symptoms that are not different from those of a regular viral bronchiolitis caused by syncytial virus. Most patients present serious bronchospasm, with hypoxemia, and in many cases they need mechanical ventilation. Physical examination is not specific. Wheezing and rhonchus can be heard bilaterally. If a patient with an adenovirus infection does not improve in 3 weeks, BO should be suspected.
After the clinical condition of the patient becomes stable, tachypnea persists, wheezing and productive cough become permanent, and oxygen saturation is reduced. Some patients with nosocomial pneumonia caused by adenovirus with an important respiratory compromise present a similar progression, requiring long hospitalizations and intensive care.
Diagnosis
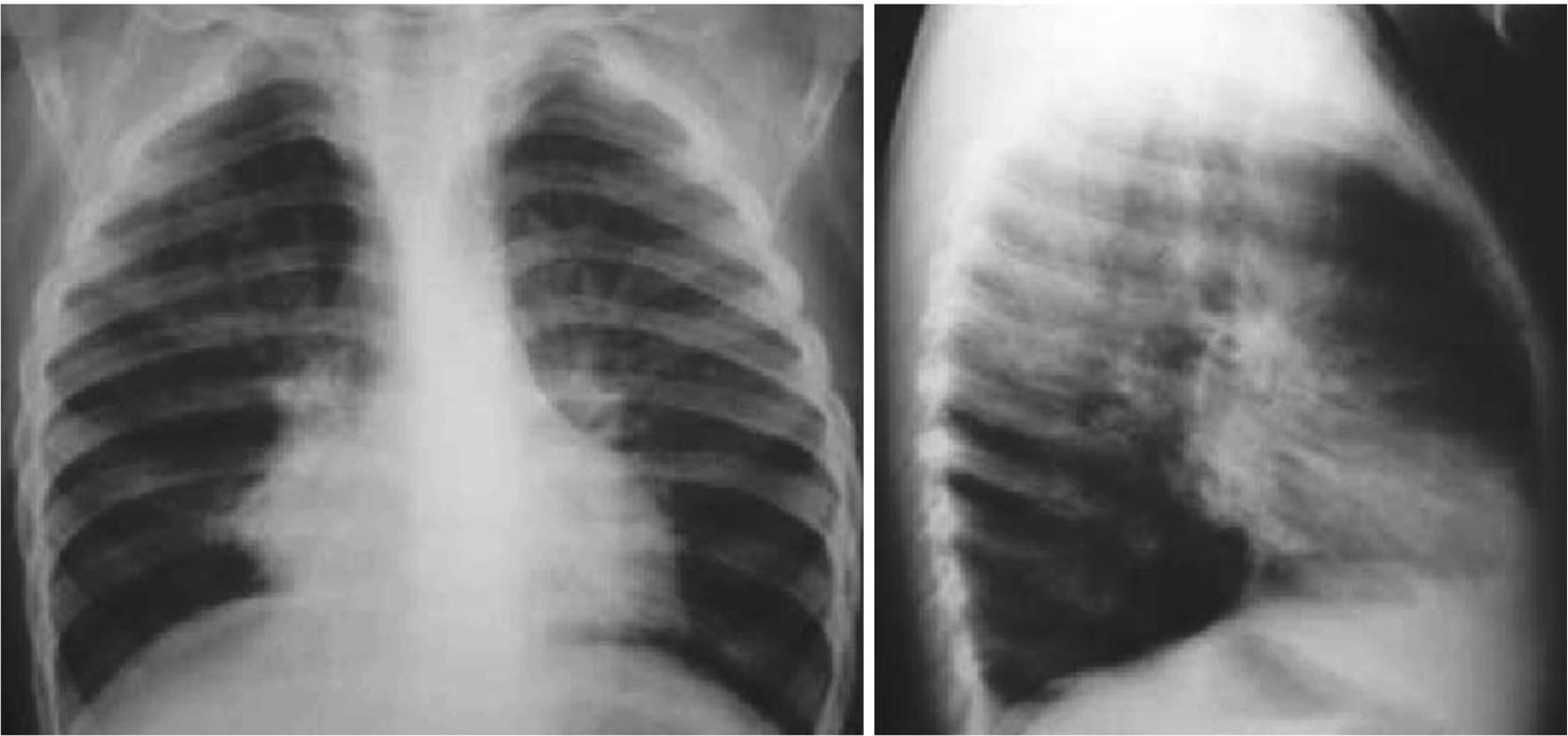
The objective of diagnosis methods is to show the obliteration of the small airway, which is an anatomopathological lesion of this disease. Because of this, lung biopsy yields the best results. Lung function tests can show severe and fixed obstruction. Indirect signs of the disease can appear in the lung images.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


