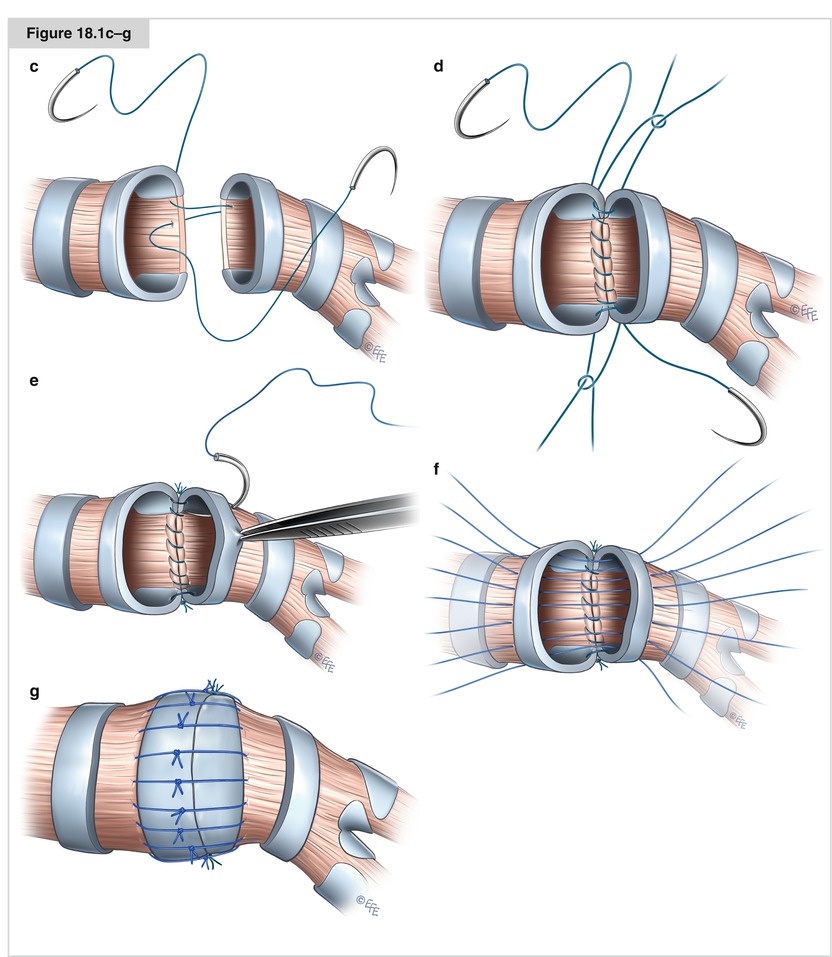
Figure 18.1a, b
Surgical technique of bronchial sleeve resection and anastomosis construction. Intraoperative management for bronchial sleeve resections follows the standards for anatomical lung resections. Airway management with a right- or left-sided double lumen tube is the procedure of choice. Alternatively, endobronchial balloon blockers may be used to achieve one-lung ventilation especially in children for whom small-size double lumen tubes are not available. For sleeve pneumonectomies or carinal resections, endobronchial high-frequency jet-ventilation may help to avoid the hassle of an over-the-field ventilation. Regarding the incision, most authors favor the standard posterolateral thoracotomy. In our experience, however, bronchial sleeve resections in conjunction with an anatomical lung resection can be most comfortably performed through an anterolateral thoracotomy. The technique of anastomosis construction predicates on whether the bronchus is approached from the anterior or posterior side. Our general surgical technique—through an anterolateral thoracotomy—is shown on the example of a left upper-lobe sleeve Resection. (a, b) Left main bronchus and lower bronchus are dissected free of adjacent tissue and transected with a knife to assure straight margins. After removal of the specimen, both bronchial margins are examined by frozen section to determine a radical resection. If one of the margins proves positive, more bronchus must be resected
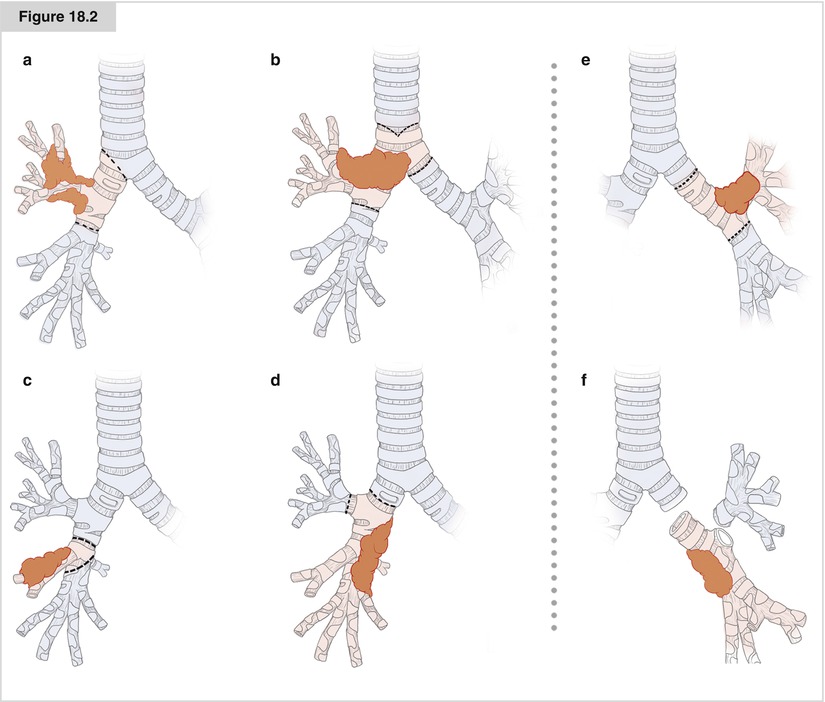
Figure 18.2
Common types of bronchial sleeve resection. This figure shows the most common types of sleeve lobectomies. Resected bronchial structures are tinted in red, preserved bronchial structures in blue. Right upper-lobe sleeve resection (a) is by far the most common sleeve lobectomy. In the Heidelberg series with over 700 bronchial sleeve resections over a period of 12 years, 45 % of all sleeve resections were right upper lobes, 35 % were left upper-lobe resections, and 8 % left lower-lobe sleeve resections. All other types combined represented just 12 % of bronchial sleeve Resections. (a) Right upper-lobe sleeve lobectomy; (b) Right upper-lobe sleeve lobectomy with inclusion of the main carina; (c) Right middle-lobe sleeve lobectomy; (d) Right lower bilobectomy with upper lobe anastomosis (Y-sleeve resection); (e) Left upper-lobe sleeve resection; (f) Left lower-lobe sleeve resection (Y-sleeve resection)
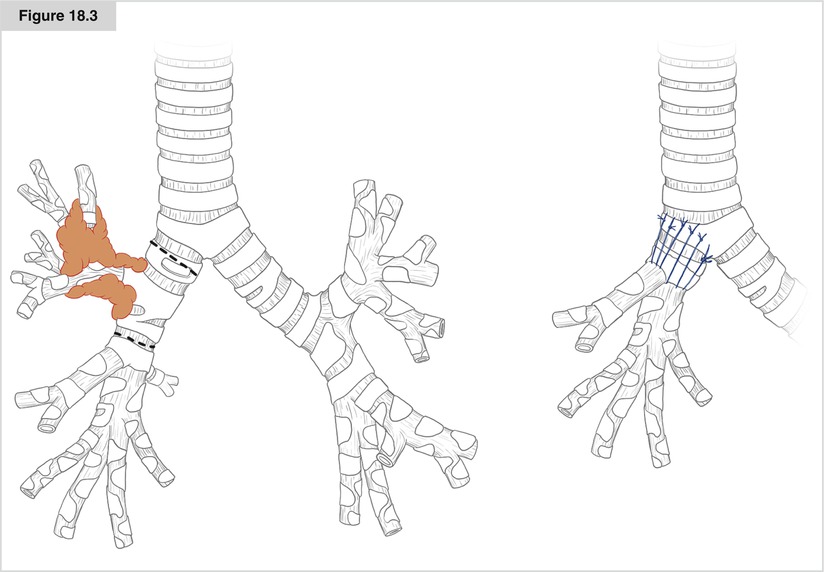
Figure 18.3
Right upper lobe sleeve resection. Tumor growth as shown in this figure with invasion of the main bronchus precludes standard right upper lobectomy. With an en bloc bronchial sleeve lobectomy, radical resection can be accomplished with avoidance of an otherwise necessary pneumonectomy. After divisions of vessels and lobar fissures as with a standard upper lobectomy, the right main and intermediate bronchi are dissected and then transected with adequate distance to the tumor. The intermediate bronchus is usually cut next to the orifice of the middle lobe bronchus to obtain bronchial ends of approximately the same caliber and to avoid having to use a long intermediate bronchus with poor blood supply for the anastomosis even if the lower border of tumor invasion is more proximal. Clear margins of both bronchi proven by frozen sections are mandatory to assure a radical resection. An end-to-end bronchial anastomosis of main and intermediate bronchi is constructed as shown in Fig. 18.1 with a running suture for the membranous portion and interrupted sutures for the cartilaginous portion. A smaller lumen disparity can be adjusted with an adapted placement of the stiches for the posterior running suture by stretching of the membranous portion of the intermediate bronchus and crimping the membrane of the main bronchus. A greater lumen disparity may require telescoping of the intermediate bronchus into the main bronchus. Telescoping, however, should be restricted to the cartilaginous portion and must include no more than one cartilage to minimize the risk for secondary stenosis. It is advisable to realize the need for telescoping before placing the first anterior stiches and adjust the distance of the stiches to the bronchial rim accordingly. Accidently occurring telescoping will result in loose sutures with subsequent leakage of the anastomosis
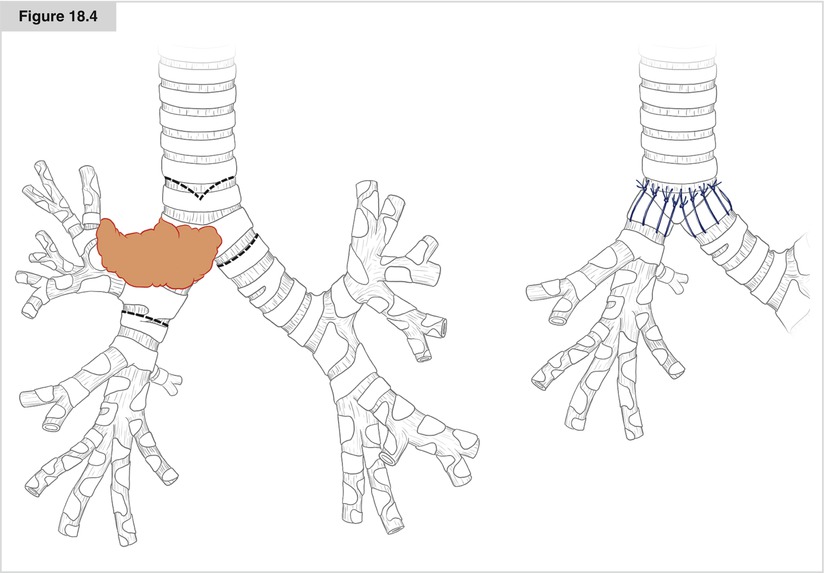
Figure 18.4
Right upper-lobe sleeve resection with main carina. For upper lobe tumors invading the proximal right main bronchus or the main carina, a bronchial sleeve resection including the main carina may be required. Resection of the main carina demands additional effort for airway management and ventilation during the procedure. In our experience, retracting the left-sided double lumen tube into the trachea and introducing an endotracheal catheter for jet ventilation into the left main bronchus manages this best. Reconstruction of the bronchial continuity results in the construction of a neo-carina of right-sided intermediate bronchus and left main bronchus with end-to-end anastomosis onto the distal trachea. Basically, two approaches can be taken. After initially constructing a side–side anastomosis of left main bronchus and right intermediate bronchus by interrupted sutures, this “double barrel” is sutured end-to-end onto the distal trachea that needs to be carved accordingly. Alternatively, an end-to-end anastomosis of the left main bronchus onto the distal trachea can be constructed first while leaving approximately one third of the cartilaginous portion open. Into this orifice, the intermediate bronchus can be sutured in an end-to-side fashion. The latter method allows for a safe repositioning of the left-sided double-lumen tube into the left main bronchus before constructing the anastomosis of the right-sided intermediate bronchus. This will safely keep the right lung down during anastomosis construction
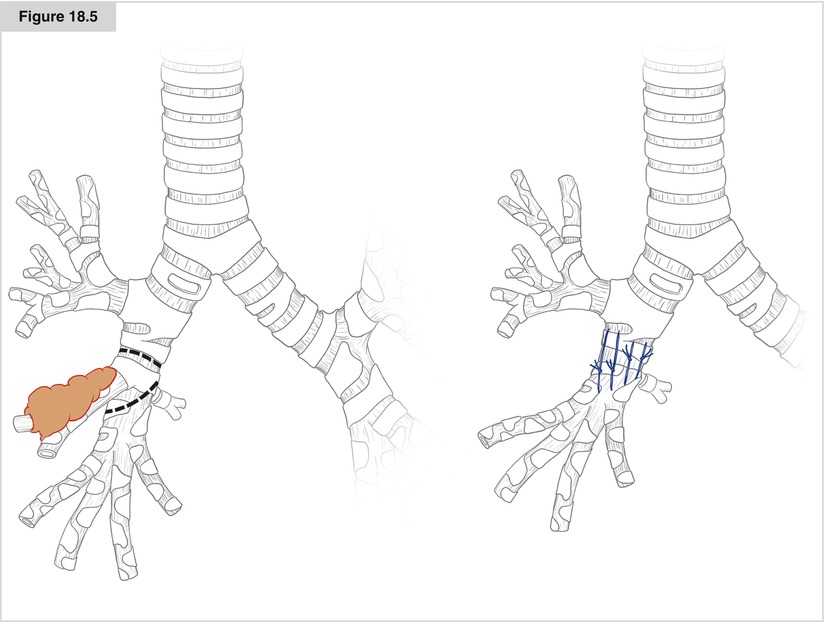
Figure 18.5
Right middle-lobe sleeve resection. Right middle-lobe bronchial sleeve resection is a rare indication in patients with non-small cell lung cancer because centrally located tumors have by then most frequently already affected adjacent lobes. However, it is a good indication for bronchial carcinoid tumors involving the orifice of the middle lobe. Loss of lung parenchyma is functionally insignificant and a radical resection with favorable long-term prognosis can be accomplished. The middle lobe bronchus is transected in conjunction with a small segment of the intermediate bronchus. Care must be taken to preserve the orifice of the segment 6 bronchus. The individual bronchial anatomy should be visualized for before transecting the intermediate bronchus and the line of the distal transection must be chosen accordingly. Most often, an oblique distal bronchial transection is required. However, this may come as no disadvantage since it helps for adjustment of lumen disparity
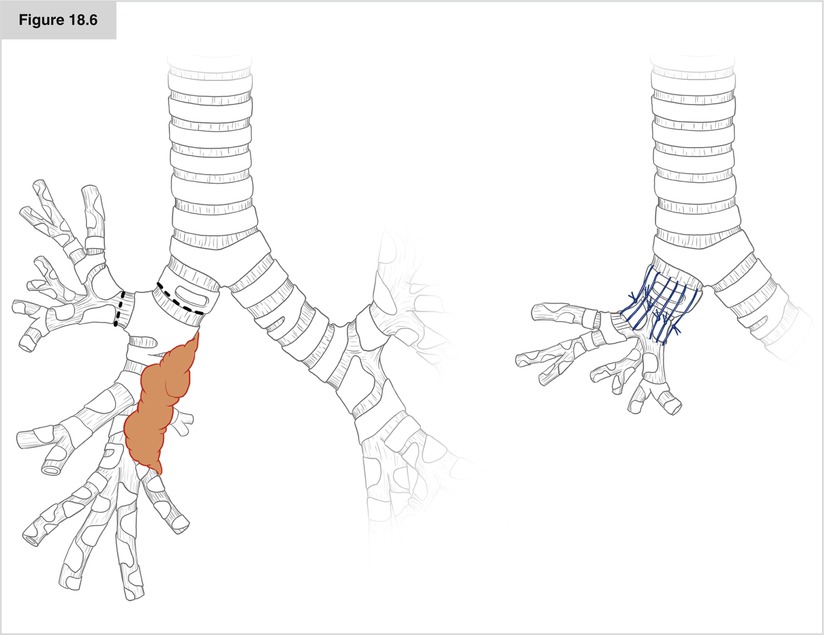
Figure 18.6




Right lower bilobectomy with sleeve resection. For lower-lobe tumors with tumor growth that extends centrally along the intermediate bronchus beyond the line for a standard lower bilobectomy, the upper lobe can nevertheless be preserved by a sleeve resection as shown here. Upper lobe bronchus and main bronchus are transected as shown. To accomplish that, the dissection however must involve the complete hilum of the right lung. In particular, the superior trunk of the pulmonary artery must be dissected and the lymph nodes along the upper lobe and intermediate bronchi must be removed. The upper lobe is then turned 90° and an end-to-end anastomosis of the upper lobe bronchus and the main bronchus is constructed. Although the upper lobe bronchus—as it is an intrapulmonary bronchus—does not exhibit the typical horseshoe-shape of the main bronchus, and often the membranous portion is very short, we basically use the same technique for anastomosis construction as shown in Fig. 18.1. A running suture is used for the posterior one third of the circumferential angle and interrupted sutures for the anterior portion. Care must be taken to protect the superior trunk of the pulmonary artery during construction of the bronchial anastomosis
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
