Bradycardias
Clinical Syndrome
Sinus node dysfunction is characterized by disorders of impulse formation in and conduction out of the sinus node (see Table 11-1). Electrocardiographically these abnormalities in sinus node function are characterized by sinus bradycardia or pauses. The most common cause of apparent sinus node dysfunction is sinus arrhythmia. Sinus arrhythmia is defined by a maximum of 160 msec difference between the shortest and longest PP intervals. Respiratory sinus arrhythmia is common in the young but dissipates with aging. It is manifested as a gradual increase in heart rate with inspiration and decrease with expiration. Sinus arrhythmia may be present in older age but in this instance is not a respiratory phenomenon. Ventriculophasic sinus arrhythmia is a unique arrhythmia associated with complete heart block. In this case the PP interval surrounding the QRS complex is shorter than the PP interval following the QRS complex (see Fig. 11-1). Heightened vagal tone (VT) from any cause can result in sinus bradycardia or pauses. Common clinical circumstances associated with vagal surges include sleep (particularly during the apneic phase of obstructive sleep apnea), nausea, vomiting, hiccups, coughing, or gagging. In the hospitalized patient on a ventilator, suctioning of the airway is a frequent cause of sinus bradycardia and pauses.
Common causes of nonvagally induced sinus node dysfunction include aging (fibrosis) and suppression by medications (e.g., β-blockers,
nondihydropyridine calcium channel blockers, digoxin, antiarrhythmic drugs, and the chronic use of lithium). Sick sinus syndrome refers to sinus node dysfunction often in association with atrial fibrillation. This commonly manifests as sinus bradycardia after conversion of atrial fibrillation. Tachybrady syndrome is similar to sick sinus syndrome (SSS) but includes other forms of supraventricular tachycardia such as atrial tachycardia. These syndromes may be associated with conduction abnormalities in the atrioventricular (AV) node as well as the sinus node.
nondihydropyridine calcium channel blockers, digoxin, antiarrhythmic drugs, and the chronic use of lithium). Sick sinus syndrome refers to sinus node dysfunction often in association with atrial fibrillation. This commonly manifests as sinus bradycardia after conversion of atrial fibrillation. Tachybrady syndrome is similar to sick sinus syndrome (SSS) but includes other forms of supraventricular tachycardia such as atrial tachycardia. These syndromes may be associated with conduction abnormalities in the atrioventricular (AV) node as well as the sinus node.
Table 11-1 Sinus Node Dysfunction | |
|---|---|
|
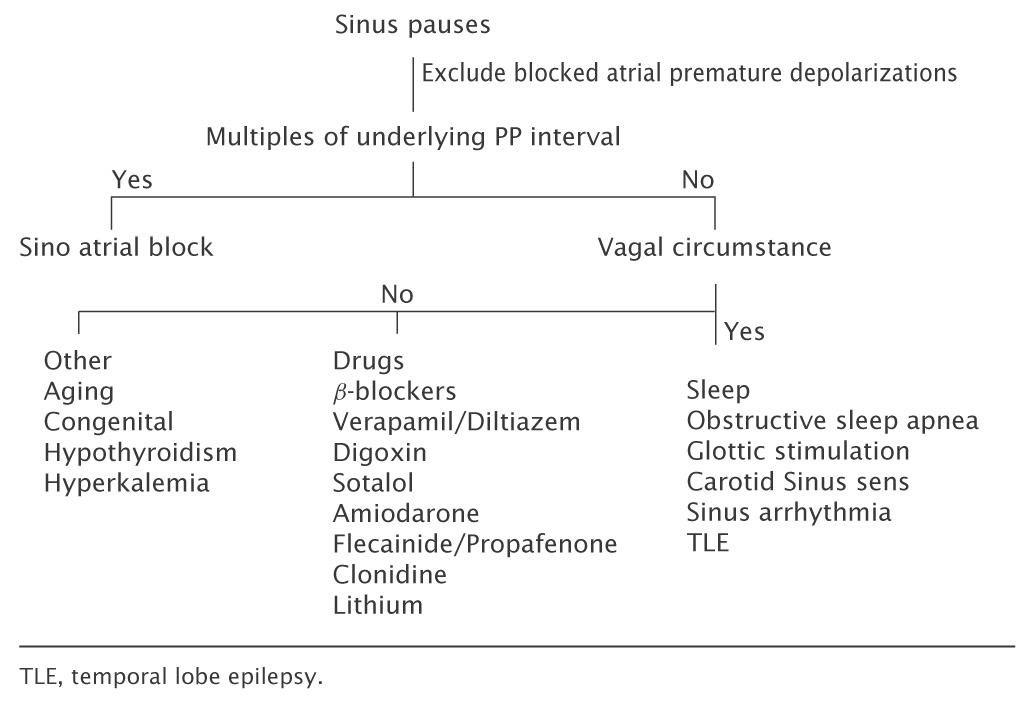
 FIGURE 11-1. Ventriculophasic conduction during complete atrioventricular (AV) block with a shorter PP interval surrounding the QRS than between the QRS complexes. |
Hypothyroidism, hyperkalemia, and hypothermia are less common causes of sinus bradycardia. Trauma to the sinus node associated with cardiac
surgery can cause sinus node dysfunction (if the right atrium is entered). This can occur in adults, particularly with redo valve surgery or in children following correction of congenital heart disease (e.g., Fontan procedure). Familial sinus node dysfunction is an autosomal dominant disorder. It is characterized by a familial pattern of sinus node dysfunction at young age (e.g., early 20s) with an associated mutation in a gene, HCN 4, which codes for a pacemaker ion channel.
surgery can cause sinus node dysfunction (if the right atrium is entered). This can occur in adults, particularly with redo valve surgery or in children following correction of congenital heart disease (e.g., Fontan procedure). Familial sinus node dysfunction is an autosomal dominant disorder. It is characterized by a familial pattern of sinus node dysfunction at young age (e.g., early 20s) with an associated mutation in a gene, HCN 4, which codes for a pacemaker ion channel.
Atrioventricular Conduction Disease
AV conduction disease can occur in the AV node or below the AV node (infranodal) within the His bundle or Purkinje system. Occasionally extrasystoles arising from the His bundle can result in AV block. These may be difficult to identify on the surface electrocardiogram (ECG) as they can conduct retrogradely to the atrium but not antegradely to the ventricle (i.e., concealed) (see Fig. 11-2). The most common causes of complete heart block are fibrocalcific degeneration (Lev disease) and idiopathic degeneration (LeNegre disease) of the conduction system, which is genetically based. A common clinical example of fibrocalcific destruction of the conduction system is heart block related to calcification of the mitral annulus. Other causes of heart block are discussed in the following text.
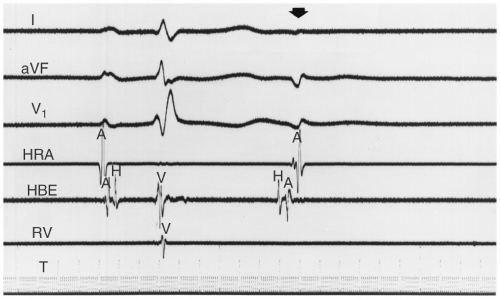 FIGURE 11-2. Demonstration of a concealed His extrasystole. A His potential precedes the atrial electrogram. The surface leads show a negative P wave in lead 2 due to retrograde conduction through the AV node. Antegrade conduction to the ventricle does not occur resulting in the absence of an associated QRS complex. AV, atrioventricular; HRA, high right atrium; HBE, His bundle electrogram; RV, right ventricular. |
Infection
Endocarditis with abscess formation in the region of the AV node and His-Purkinje system (HPS) can result in conduction abnormalities including heart
block. Abscesses involving the right and noncoronary cusp regions of the aortic valve are most often responsible for conduction abnormalities due to invasion of the AV node (noncoronary cusp) or proximal HPS (right coronary cusp). Lyme disease is an important cause of AV nodal block, which presents as a secondary manifestation of infection. It rarely if ever involves the infranodal conduction system and is generally reversible with antibiotic treatment.
block. Abscesses involving the right and noncoronary cusp regions of the aortic valve are most often responsible for conduction abnormalities due to invasion of the AV node (noncoronary cusp) or proximal HPS (right coronary cusp). Lyme disease is an important cause of AV nodal block, which presents as a secondary manifestation of infection. It rarely if ever involves the infranodal conduction system and is generally reversible with antibiotic treatment.
Acute myocarditis can present with complete heart block in any region of the conduction system. When this occurs it is usually accompanied by a fulminant myocarditis which may or may not recover.
Infiltrative diseases such as sarcoidosis and benign tumors such as rhabdomyomas or malignancy can cause conduction disease.
Congenital Atrioventricular Block
Congenital AV block may be associated with maternal systemic lupus erythematosus (with anti-Rho and anti-La antibodies) or may occur as an independent entity. It causes AV nodal conduction disease ranging from a prolonged PR interval to complete heart block. It is increasingly recognized in infancy with improved prenatal diagnostic testing. It is not unusual for prolonged AV nodal Wenckebach periodicity or 2:1 block to persist for years and then deteriorate into complete heart block. Patients will often present with diminished exercise tolerance. Predictors of mortality in these patients include ventricular ectopy particularly in association with a prolonged QT interval, mitral regurgitation, and progressive left ventricular dysfunction.
Corrected (L type) transposition of the great vessels is associated with complete heart block. Some forms of familial dilated cardiomyopathy are also associated with progressive conduction disease. In this latter disorder the conduction disease may present in early adulthood and precede the development of ventricular dysfunction.
Neurodegenerative Disorders
Myotonic dystrophy is the most common neurodegenerative disease associated with conduction disease. It is an autosomal dominant disorder associated with the development of an infranodal conduction abnormality (without cardiomyopathy). These patients can develop complete heart block as well as ventricular tachycardia due to bundle branch reentry. Conduction disease may present with modest PR prolongation or the new development of a fascicular or bundle branch block (BBB).
Emery Dreifuss syndrome is a severe form of X-linked muscular dystrophy associated with complete heart block, atrial fibrillation, and dilated cardiomyopathy. Duchenne and Beckers muscular dystrophy are also associated dilated cardiomyopathy and varying degrees of AV conduction abnormality and atrial dysrhythmias. Limb Girdle muscular dystrophy is also associated with
AV conduction disease. Other forms of neuromuscular disease associated with conduction abnormalities include Erb dystrophy and Kearns-Sayre syndrome.
AV conduction disease. Other forms of neuromuscular disease associated with conduction abnormalities include Erb dystrophy and Kearns-Sayre syndrome.
Heart Block Associated with Trauma
The AV node or His bundle can be damaged during aortic valve surgery. Mitral valve surgery may result in damage to the His bundle. This damage may be permanent or reversible if due to edema. The physicians typically wait 4 to 7 days for recovery of conduction before placing a permanent pacemaker in these patients. Closure of ventricular septal defects (VSDs), whether surgical (particularly with AV canal repairs) or catheter-based can also result in HPS damage.
Paroxysmal Atrio Ventricular Block
This disorder is characterized by the abrupt development of AV block associated with the slowing of impulses reaching the HPS. This can be due to slowing of the sinus rate following premature atrial, His, or ventricular beats, or during posttachycardia pauses (see Fig. 11-3). It is an important cause of unrecognized syncope and is a manifestation of infranodal conduction disease that caused phase 4 depolarization in abnormal tissue.
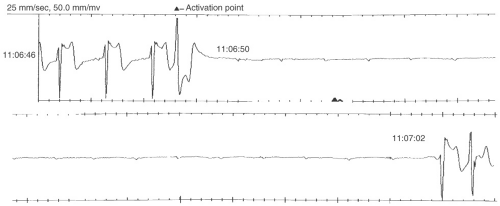 FIGURE 11-3. Ventricular premature depolarization results in paroxysmal atrioventricular (AV) block. |
Conduction Disease Associated with Myocardial Infarction
The conduction disease associated with inferior myocardial infarction (IMI) occurs in two main stages. High-degree AV block, even associated with sinus tachycardia, may be seen in the first 24 hours following infarction (see Figs. 11-4 and 11-5). This is likely due to the Bezold Jarsch reflex and is
atropine sensitive. A second, later stage begins day 2 or 3 after myocardial infarction (MI) and occurs in a predictable sequence (PR prolongation, followed by type 1 second degree AV block followed by complete heart block). These abnormalities occur predominantly with occlusion of the proximal right coronary artery (RCA) and may have concomitant right ventricular (RV) infarction. Occlusion of the sinus node branches of the RCA can rarely result in sinus bradycardia or atrial fibrillation. More often sinus bradycardia results from heightened Vagal tone. The RCA supplies the AV node, which may produce PR prolongation, Mobitz 1, and complete heart block with a narrow complex escape rhythm. Conduction abnormalities present within the first few hours of infarction and are due to ischemia and heightened Vagal tone. Abnormalities that persist beyond 24 to 48 hours are due to edema and almost always normalize after 7 to 10 days. In this setting, the loss of AV synchrony can result in significant hemodynamic compromise. Temporary pacing may be helpful but the risk of RV perforation must be considered.
atropine sensitive. A second, later stage begins day 2 or 3 after myocardial infarction (MI) and occurs in a predictable sequence (PR prolongation, followed by type 1 second degree AV block followed by complete heart block). These abnormalities occur predominantly with occlusion of the proximal right coronary artery (RCA) and may have concomitant right ventricular (RV) infarction. Occlusion of the sinus node branches of the RCA can rarely result in sinus bradycardia or atrial fibrillation. More often sinus bradycardia results from heightened Vagal tone. The RCA supplies the AV node, which may produce PR prolongation, Mobitz 1, and complete heart block with a narrow complex escape rhythm. Conduction abnormalities present within the first few hours of infarction and are due to ischemia and heightened Vagal tone. Abnormalities that persist beyond 24 to 48 hours are due to edema and almost always normalize after 7 to 10 days. In this setting, the loss of AV synchrony can result in significant hemodynamic compromise. Temporary pacing may be helpful but the risk of RV perforation must be considered.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


