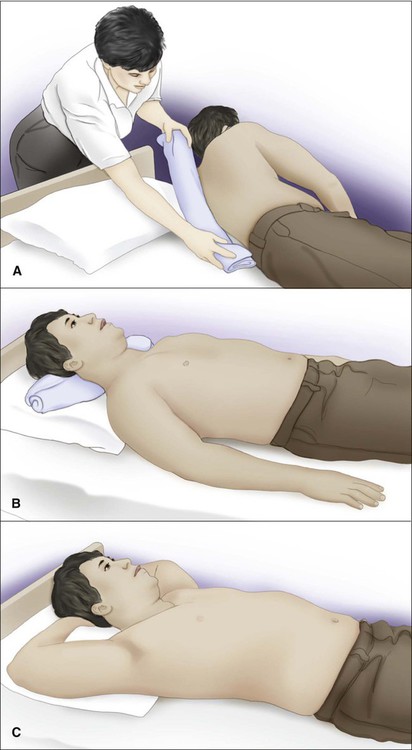
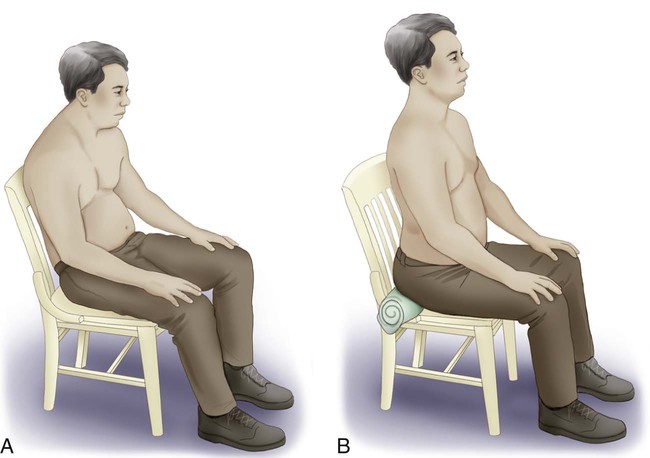
Body mechanics can be defined as the efficient use of one’s body as a machine and locomotive entity. When working with critically ill or chronically dependent patients, physical therapists frequently change patients’ body positioning before and during treatments to facilitate ventilatory potential and improve patient outcomes. Therapists and nurses attempting to position or move dependent patients need to understand and use proper body mechanics.1–5 This knowledge is necessary to maximize treatment outcomes and to reduce biomechanical stress and trauma for the patient and for those working directly with the patient. Low back pain is the most common cause of work-related disability among employees younger than 46 years, and nurses and physical therapists account for over half of the annual prevalence of low back pain among health care personnel.6,7 Positioning and moving dependent patients is an art that is quite different from working with a patient who can move independently and assume any given position with ease. In this chapter, the principles of body positioning and moving dependent patients are discussed. Because of the three-dimensional nature of breathing, one of the therapist’s most important goals is to facilitate chest excursion in all three planes of ventilation: anterior-posterior, superior-inferior, and lateral.8 This can be accomplished by improving the length-tension relationships of the muscles used in inspiration.9,10 Massery8 reasons that proper positioning to enhance inspiratory muscles will accomplish the following: 1. Improve the length-tension relationship of the accessory ventilatory muscles involved in that posture. 2. Incorporate a passive stretch of the chest wall. 3. Use the natural coordination of the trunk-chest wall movement with inspiration and exhalation patterns to maximize movement. The following are some common improvements that can be incorporated into normal positioning. Upper chest expansion can be increased by removing pillows from under the patient’s head to increase thoracic extension. This will increase the length-tension relationship of the neck accessory muscles (scalene and sternocleidomastoid muscles). Increased movement will be noted in the upper chest in the superior and anterior planes.8 Further anterior expansion may be achieved with a towel roll placed longitudinally at the vertebral spine to open the anterior chest of a patient who tends toward excessive flexion of the trunk (Figure 42-1, A). If the patient needs support under the head to achieve a neutral chin tuck to protect swallowing ability, a thin pillow or horizontal towel roll under the occiput can be used (Figure 42-1, B). External rotation of the shoulders with the scapulae in a neutral or retracted position will stretch the pectoralis and intercostal muscles. This may improve lateral and anterior chest wall movements.10,11 If a patient has full range of motion (ROM) and is comfortable with the arms placed overhead or in full flexion/abduction/external rotation for maximal stretch, this is the optimal position for potential maximal excursion of the anterior chest wall (Figure 42-1, C). If there are major shoulder limitations, moderate shoulder abduction with forearm supination may be the best position available to facilitate chest excursion. Whenever significant limitations are found, the therapist should try to modify the position to accommodate the patient’s needs and achieve optimal ventilation. Side-lying is an optimal position that may improve breathing patterns. At the same time, medical professionals should continue to heed the need for prescriptive rather than routine patient positioning. In side-lying, gravity is eliminated for anterior expansion and the diaphragm moves freely, particularly the upper hemi-diaphragm, which is not having to shift the abdominal contents as much as the lower hemi-diaphragm. Such a position may be optimal for preterm infants who, when placed in a side-lying or prone position, have been shown to have fewer stress behaviors, resulting in longer periods of sleep with less fussiness and crying.12 However, side-lying positions can also result in decreased forced vital capacity and forced expiratory volume lung measurements and may not be optimal for patients with risks for cardiopulmonary compromise.13 A specific example of the need for prescriptive rather than routine positioning of a patient in side-lying involves a patient with pneumonia or atelectasis. If a patient has right lower lobe pneumonia or atelectasis, side-lying on the unaffected left side will improve oxygenation. Conversely, side-lying with the affected side down will cause a decrease in oxygenation (differential shunt) because a patient with decreased ventilation receives more perfusion to the down lung with more shunting. Prone positioning can improve oxygenation with minimal untoward effects in several patient populations, including those who are critically ill and medically unstable, such as preterm infants, patients with acute respiratory distress syndrome (ARDS), and patients with hypoxemic acute respiratory failure.12,14–23 Oxygenation is improved with prone positioning when compared with supine positioning via more homogenous lung inflation and alveolar ventilation,24 but some cases with concomitant difficulties have been reported. One instance of severe hypotension was noted in a child with scoliosis, pectus excavatum, and neurofibromatosis who presented for a spinal fusion. It is recommended that sternal pressure be avoided in patients with chest wall deformities.25 Early enteral nutrition is poorly tolerated in critically ill patients receiving invasive mechanical ventilation in the prone position. Medication can be given to enhance gastric emptying and prevent vomiting. Feeding the patient in the prone position becomes challenging if the patient is mechanically ventilated as well.26 When a patient is mechanically ventilated and has numerous tubes and monitors, turning him or her to the prone position takes planning and is staff intensive. Although turning a patient prone may be difficult, reviews of related studies report that prone positioning may reduce the absolute mortality of severely hypoxemic ARDS patients by approximately 10% in addition to improving their oxygenation by 27%-39%. However, the reviews also suggest that long-term prone positioning can expose patients with less severe ARDS to unnecessary increased risks for pressure ulcers, endotracheal tube obstruction, and chest tube dislodgement.24,27 Thus body positioning requires careful prescription of not only the specific positions, but also the time the patient spends in those positions, which is largely response dependent. Pelvic alignment is a key component to optimal posture. A relatively anterior tilted pelvis in healthy, flexible adults may reduce the kyphotic curve in the thoracic spine, adduct the scapulae toward a neutral position, produce a more neutral or externally rotated upper-extremity position, and pull the head back into a neutral chin tuck.28,29 The anterior tilt of the pelvis may improve upper-extremity ROM and ventilation. Attending to this one consideration may be all that is needed to improve the breathing capacity of some patients, allowing them to continue to advance in their exercise programs or rehabilitation. Further benefit may be achieved with a lumbar roll. Another simple means of attaining an anterior pelvic tilt in sitting is to have the patient lean forward over his or her legs, then slide a towel roll horizontally just behind the ischial tuberosities, which can prevent the pelvis from tilting posteriorly (Figure 42-2).30 This can be well tolerated by patients with intact sensation and a pelvis that is at least minimally mobile. For patients with neurological impairment who have impaired sensation or less pelvic mobility, a wedge can be substituted; however, some sliding may occur. In addition to a relatively anteriorly tilted pelvis, a posture of anterior trunk inclination (forward-lean) with arm bracing has been shown to increase ventilatory capacity.31 Such positioning has resulted in higher values of maximal respiratory pressures and respiratory muscle endurance in patients with chronic obstructive pulmonary disease.32
Body Mechanics
Positioning and Moving Patients
Positioning for Optimal Ventilation
Supine Position
Side-Lying Position
Prone Position
Upright Postures
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Body Mechanics: Positioning and Moving Patients