Figures 33.1 and 33.2
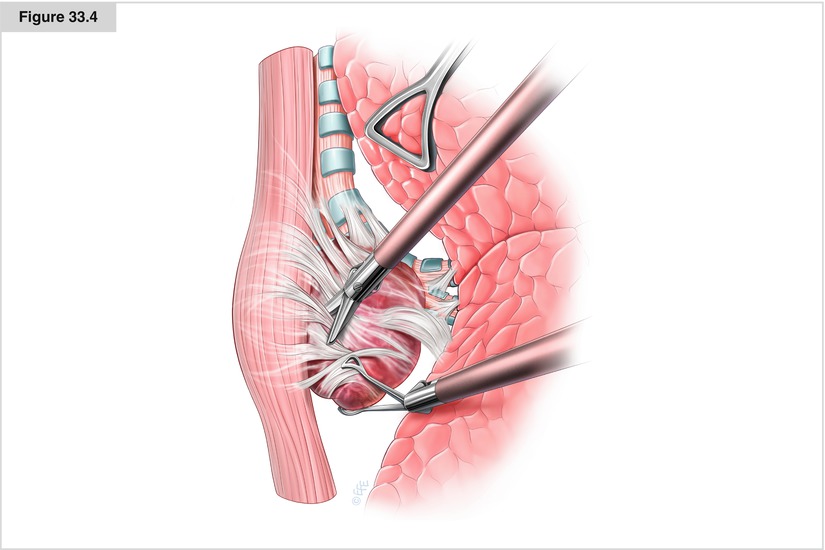
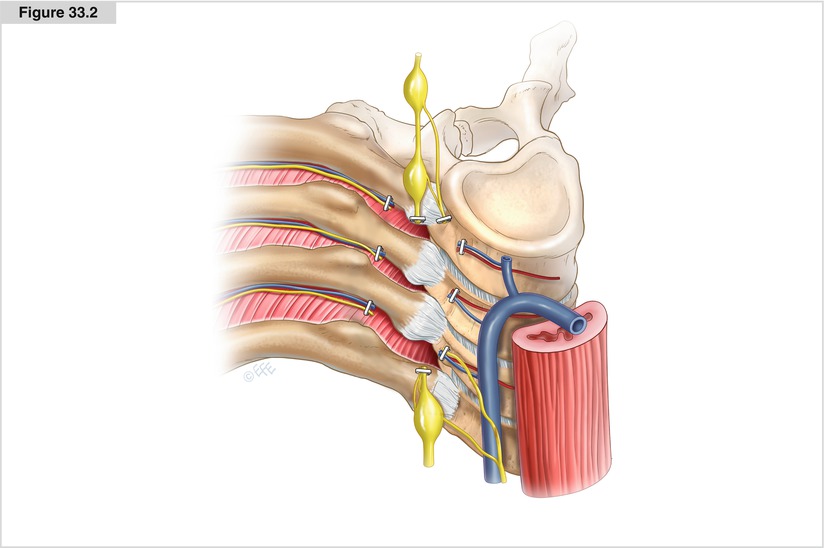
If an intraspinal extension of the neurogenic tumor can be safely excluded, it may be assumed that the tumor can be removed completely by thoracoscopy. An exception is the occasional tumor that has broad contact with the pleural apex, requiring an additional axillary incision via the second intercostal space under certain circumstances. The lesion is always covered by the parietal pleura; it rests mostly with a wide base on the intervertebral foramina, thus it is not very mobile. If the surgeon prefers to stand with a ventral view, the patient is placed in the lateral decubitus position and tilted slightly posteriorly. Three to four incisions are made in the midaxillary line for placement of the video-optic, manipulation forceps, and lung retractor. The parietal pleura is cut in circular fashion around the base of the tumor; accurate and thorough hemostasis is of utmost importance to prevent hematoma of the pleura, which would considerably complicate the overall view of the operative field. The blood vessels accompanying the intercostal nerves are clipped anterior and posterior to the tumor. The sympathetic chain proximal and distal to the neurogenic tumor also must be clipped. Then the tumor is mobilized at its base, step by step, by blunt dissection while being manipulated with only a swab; to prevent injury to the capsule, the tumor must not be treated roughly. After complete excision, the tumor is placed into an endosurgical extraction bag and removed from the pleural cavity
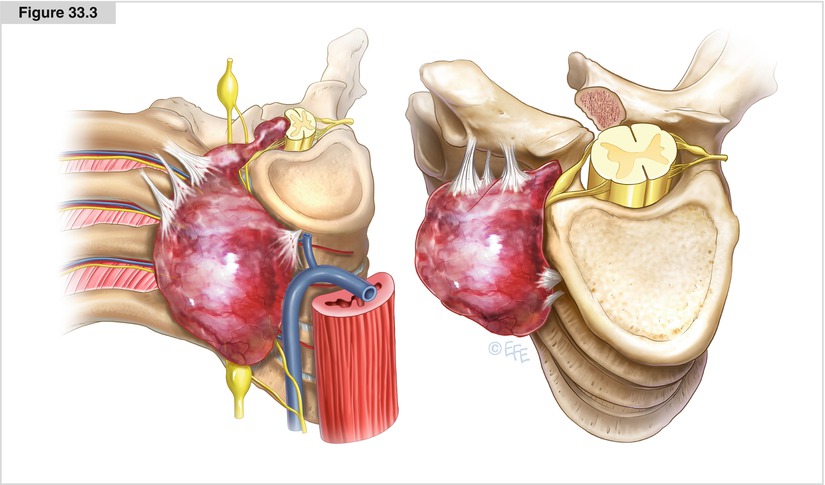
Figure 33.3
Neurogenic tumors may widen the intervertebral foramen without spreading into the canal. This constellation also permits a complete tumor extension alone from the thoracic cavity; however, tearing of the nerve root may have disastrous consequences, namely direct injury to the spinal cord, laceration of the attendant intercostal artery, or dura injury resulting in a loss of cerebrospinal fluid. Placement of a clip before the spinal root is severed prevents the dura from opening. With regard to dumbbell tumors, various strategies have been implemented successfully, including a neurosurgical/thoracic procedure in one or two operations as well as in toto tumor removal by means of a posterolateral thoracotomy (Bousamra et al. 2008). Because it can be determined intraoperatively whether a tumor is completely extradural and can be removed without opening the dura, or whether an intradural extension is exhibited, neurosurgical expertise should always be readily available