In a woman with sinus rhythm a couplet of ventricular premature complexes is followed by a retrograde P wave. A subsequent couplet of ventricular premature complexes is followed by typical atrioventricular nodal reentrant tachycardia.
A 52-year-old-woman was seen in the office for follow-up of coronary artery disease. She reported intermittent episodes of lightheadedness. An electrocardiogram ( Figure 1 ) demonstrated paroxysms of supraventricular tachycardia, with a rate of 191 beats/min. Although the patient was referred for further evaluation, she was lost to follow-up. Without an electrophysiologic study of the arrhythmia, we have postulated the mechanism for its initiation.
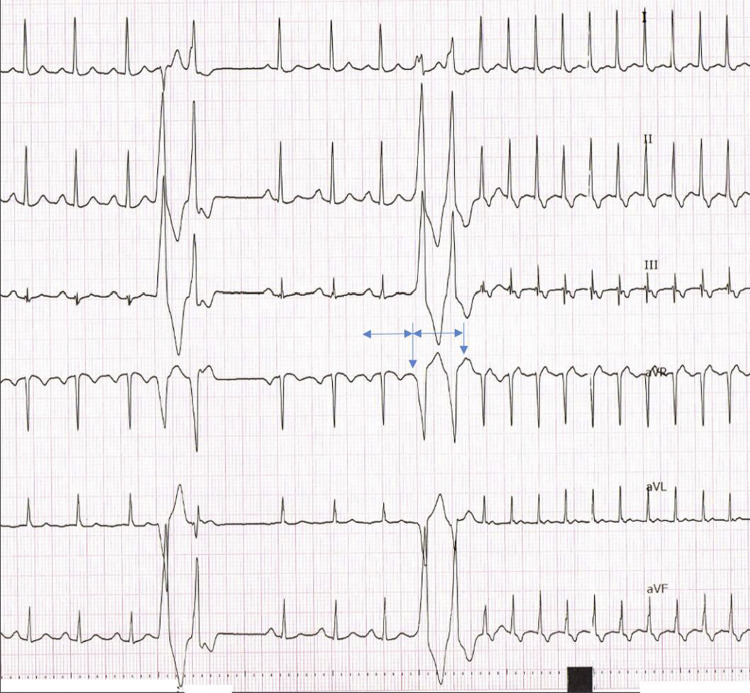
The fourth, fifth, ninth, and tenth complexes are ventricular premature complexes (VPCs). After the 10th complex, a short RP (∼60 ms), narrow complex tachycardia ensues, likely representing typical (slow-fast) atrioventricular nodal reentrant tachycardia (AVNRT).
A P wave can be seen after the second VPC, which likely represents retrograde atrial activation through the fast pathway. The sinus rate is then marked by the horizontal double-headed arrows. Just preceding the ninth QRS (first VPC of the second couplet), the onset of a sinus P wave can be seen (long vertical arrow). This sinus P renders the fast pathway refractory and no retrograde activation of the atrium follows the third VPC.
After the fourth VPC, a P wave is evident within the T wave (short vertical arrow). This P wave is in time with the sinus rate. After this, a short RP tachycardia is initiated, with P waves evident immediately after each QRS complex. The form is that of typical AVNRT, or “down the slow, up the fast,” as suggested by the short RP interval.
The first QRS complex of the tachycardia appears attenuated. It is possible that this occurs due to partial refractoriness of the AV node caused by the previous sinus activation. Thus, retrograde activation is slowed and ultimately results in atrial activation occurring simultaneously with the first QRS of tachycardia. The superimposed P wave attenuates the QRS complex. This does not occur with subsequent beats of tachycardia, and thus, they appear normal.
VPCs are more commonly observed to initiate atypical AVNRT due to retrograde slow pathway conduction when the fast pathway is refractory and unexcitable, that is, the effective refractory period of the fast pathway is usually longer than that of the slow pathway. Initiation of typical AVNRT with a VPC is less commonly observed, but as Sung et al first demonstrated in 1978, typical AVNRT may occur as long as the retrograde effective refractory period of the fast pathway is shorter than that of the slow pathway. This property permits a retrograde impulse from a VPC, at a cycle length of approximately 320 ms in this case (the RR interval of the 2 VPCs), to travel retrograde up the fast pathway and anterograde down the slow pathway, causing first an isolated retrograde P wave and then sustained typical AVNRT.
Disclosures
The authors have no conflicts of interest to disclose.
See page 936 for disclosure information.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


