Atrial fibrillation is the most common cardiac arrhythmia necessitating hospitalization in the United States (1). Although not immediately life-threatening, atrial fibrillation is associated with significant rates of morbidity and mortality. Furthermore, recurrences of arrhythmia and complications from therapy present a challenge for both the patient and the clinician.
USUAL CAUSES
Based on the current clinical and experimental data, probably multiple mechanisms are responsible for initiating and maintaining atrial fibrillation. Classically, atrial fibrillation is thought to be perpetuated by the presence of multiple self-sustaining waves of atrial depolarization, or wavelets (2,3). In recent years, the concept of drivers and rotors has been proposed as a major mechanism in the pathophysiology of AF. When the rapid periodic activity of a rotor encounters atrial tissue incapable of maintaining 1:1 activation, fibrillatory conduction results. The rotor hypothesis predicts that a frequency gradient exists between the source and more remote atrial tissue. Indeed, evidence of left-to-right gradients has been reported in both animal models (4) and clinical studies (5). Whatever the mechanism, as episodes of atrial fibrillation become more frequent or long lasting, electrophysiologic and structural properties of the atrium are altered and become maladaptive. Although atrial fibrillation may be paroxysmal, or self-terminating, the remodeling process may result in atrial fibrillation becoming persistent or chronic, which indicates that either pharmacologic or electrical conversion (i.e., cardioversion) is required to restore sinus rhythm.
Approximately 1% to 2% of the general population has atrial fibrillation; however, the prevalence of atrial fibrillation increases with age from less than 1% among persons younger than 50 years up to 9% for those older than 80 years (6,7). No distinct preponderance occurs with regard to gender.
Atrial fibrillation has a significant association with structural heart disease (Table 17.1). Twenty-five percent of patients with atrial fibrillation also have concomitant coronary artery disease (7). Although only about 10% of all myocardial infarctions are associated with atrial fibrillation, its presence is associated with a mortality rate of up to 40% (8). One third of patients undergoing coronary artery bypass grafting experience atrial fibrillation, usually around the third postoperative day. Although it usually terminates spontaneously, postoperative atrial fibrillation adds to hospital length of stay and cost.
The association of atrial fibrillation and valvular heart disease is well established. Rheumatic valvular disease greatly increases the chance of developing atrial fibrillation and quadruples the risk of thromboembolic complications. Of the patients with left ventricular dysfunction, approximately one in five have atrial fibrillation (9). This arrhythmia may also be part of the initial presentation of acute pericarditis and rare cardiac tumors, such as atrial myxoma.
TABLE 17.1.Cardiac and noncardiac conditions associated with atrial fibrillation
Cardiac diseases associated with atrial fibrillation
Coronary artery disease
Dilated cardiomyopathy
Hypertrophic cardiomyopathy
Valvular heart disease
Rheumatic
Nonrheumatic
Cardiac arrhythmias
Atrial tachycardia
Atrial flutter
Atrioventricular nodal reentrant tachycardia
Wolf-Parkinson-White syndrome
Sick sinus syndrome
Pericarditis
Noncardiac disease associated with atrial fibrillation
Systemic hypertension
Diabetes mellitus
Hyperthyroidism
Pulmonary diseases
Chronic obstructive pulmonary disease
Primary pulmonary hypertension
Acute pulmonary embolism
Adapted from: Pelosi F, Morady F. Evaluation and management of atrial fibrillation. Med Clin North Am 2001;85:225-244, with permission.
Other cardiac arrhythmias, such as those related to the Wolff-Parkinson-White syndrome, may be associated with atrial fibrillation. Catheter ablation of the accessory pathway that causes this syndrome also eliminates atrial fibrillation in 90% of cases (10). Other arrhythmias associated with atrial fibrillation include atrial tachycardia, atrioventricular nodal reentrant tachycardias, and bradyarrhythmias, such as sick sinus syndrome and other sinus node dysfunction.
Atrial fibrillation is associated with otherwise noncardiac systemic diseases. Systemic hypertension is found in 45%, and diabetes mellitus in 10%, of patients with atrial fibrillation (7). Although associated thyroid disease accounts for about 2% of cases of atrial fibrillation, it is one of a few reversible causes of this arrhythmia and should not be overlooked (11). The presence of atrial fibrillation and chronic obstructive pulmonary disease is associated with an increased rate of mortality. Patients with acute pulmonary embolism may present with atrial fibrillation.
No apparent cause may be identified in approximately 3% of patients with atrial fibrillation (12). This lone atrial fibrillation is not associated with a high thromboembolic risk in younger age groups, but as a person ages or other associated conditions develop, the risk may increase.
SIGNS AND SYMPTOMS
The presenting symptoms of atrial fibrillation are quite variable. Palpitations, fatigue, or dyspnea with exertion are common. Atrial fibrillation may exacerbate symptoms of cardiac ischemia in the presence of underlying coronary artery disease. Loss of atrial contractile function during atrial fibrillation reduces cardiac output and may lead to congestive heart failure in patients with left ventricular dysfunction. Atrial fibrillation rarely causes syncope; therefore, syncope attributed to such a diagnosis should be called into question. Asymptomatic episodes may occur in otherwise symptomatic patients with atrial fibrillation; therefore, reliance on symptoms may underestimate the arrhythmic burden attributable to atrial fibrillation (13).
History and physical examination of a patient with atrial fibrillation should first be directed at determining the degree of clinical compromise (Table 17.2). The pulse is classically described as “irregularly irregular,” but a very rapid ventricular rate may make this difficult to detect. Blood pressure is typically normal, and hypotension is unusual in the absence of left ventricular outflow tract obstruction. The clinician should look for signs of congestive heart failure such as pulmonary rales, a third heart sound (S3), or peripheral edema. Cardiac auscultation may reveal cardiac murmurs, right ventricular lift, or displaced point of maximum impulse, suggestive of structural heart disease.
TABLE 17.2.Components of clinical evaluation of atrial fibrillation
COMPONENT
FINDINGS
History
Determine duration of atrial fibrillation
Determine severity of symptoms
Palpitation
Fatigue
Dyspnea, particularly on exertion
Lightheadedness
Identify symptoms of ischemia or congestive heart failure (CHF)
Physical examination
Pulse: rate and irregularity
Vital signs
Blood pressure
Neck
Jugular venous distention
Pulmonary
Rales suggestive of CHF
Cardiac
S3 gallop suggestive of CHF
Presence of murmurs suggestive of valvular disease
Identify ischemia, left ventricular preexcitation, preexcitation syndromes (Wolff-Parkinson-White syndrome)
Echocardiography
Left ventricular function, valvular function, outflow obstruction, cardiac chamber size
Exercise testing
Identify cardiac ischemia
Determine adequacy of rate control
Ambulatory monitoring
Determine adequacy of rate control
Correlate symptoms with arrhythmia
HELPFUL TESTS
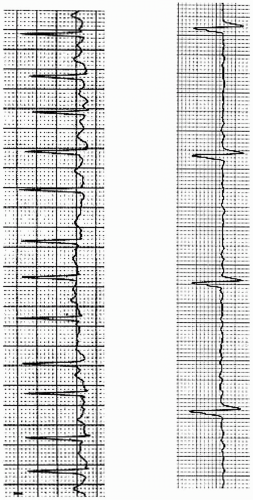
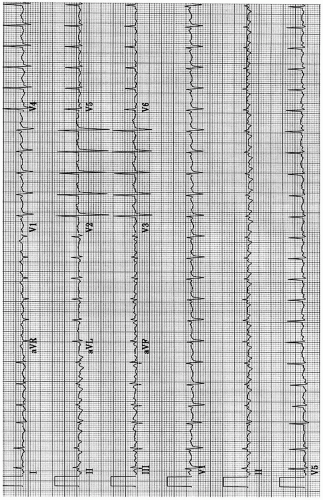
Electrocardiography is the most helpful means of establishing a diagnosis of atrial fibrillation. The electrocardiogram is characterized by an irregular ventricular rate with no clear pattern (“irregularly irregular”), although this may be obscured by rapid rates (Fig. 17.1). Replacement of the normal P waves with disorganized, fibrillatory atrial activity is the hallmark of atrial fibrillation but may be concealed by artifact or rapid ventricular rates. In the presence of complete atrioventricular block, the ventricular rate can be regular. The diagnosis of classic atrial flutter is made by the presence of flutter waves, a more organized atrial activity appearing as a regular sawtooth pattern of atrial activity best seen in the inferior limb leads II, III, and aVF (Fig. 17.2). Ventricular rates are typically regular at a fixed ratio to the flutter rate (e.g., 2:1, 3:1); however, variable block in the atrioventricular node can result in variable ventricular rates. The presence of ST-segment or T-wave abnormalities may suggest ischemia or treatment with digitalis. Prolongation of the QRS duration can be suggestive of distal conduction system disease, left ventricular hypertrophy, or preexcitation syndromes such as Wolff-Parkinson-White syndrome.
Chest radiography may identify abnormalities in cardiac silhouette or confirm the presence of pulmonary congestion.
Echocardiography is helpful for identifying associated structural heart disease and guiding management in patients with atrial fibrillation. Associated conditions such as valvular heart disease or cardiomyopathy may be revealed, which have significant impact on treatment decisions. The presence of significant left atrial enlargement is associated with a low likelihood of maintenance of normal rhythm over the long term (14).
FIGURE 17.1. Top: A patient with atrial fibrillation. Note the fibrillatory atrial activity Bottom: Atrial fibrillation with complete heart block. Although atrial fibrillation is clearly present, complete heart block with ajunctional escape rhythm results in a regular ventricular rhythm.
FIGURE 17.2. A 12-lead electrocardiogram showing with atrial flutter and 2:1 atrioventricular conduction. The “sawtooth” pattern of the flutter waves is best seen in leads II, III, and aVF.
Exercise testing should be considered for patients with coronary risk factors or anginal symptoms. Exercise testing may also be used to determine the adequacy of ventricular rate control during initial presentation and therapy. In addition, stress testing may be helpful in selecting an antiarrhythmic agent in patients with symptomatic atrial fibrillation. For example, if large perfusion defects or other evidence of coronary disease are found on noninvasive testing, class IC agents (e.g., propafenone, flecainide) should be avoided because of the risk of ventricular proarrhythmia.
COMPLICATIONS
Although not immediately life-threatening, atrial fibrillation has several complications associated with increased rates of morbidity and mortality. In some patients with the Wolff-Parkinson-White syndrome and rapidly conducting accessory pathways that bypass the atrioventricular node, a very rapid ventricular rate during atrial fibrillation with ventricular preexcitation may lead to ventricular fibrillation and sudden death (Fig. 17.3). For this reason, radiofrequency ablation of the accessory pathway is recommended when ventricular preexcitation during atrial fibrillation is present. Atrial fibrillation with rapid ventricular rates associated with left ventricular outflow tract obstruction or mitral stenosis may lead to hypotension and rapid clinical deterioration. Similar complications may occur with atrial flutter with rapid ventricular rates. Uncontrolled rapid ventricular rates may be associated with left ventricular dysfunction and heart failure related to a persistently elevated heart rate (15,16).
Of the more common complications of atrial fibrillation, the most devastating is that of thromboembolism, especially stroke. Stroke attributed to atrial fibrillation is associated with death or severe debilitation at a rate twice that of stroke from other causes (17,18). The incidence of stroke increases with age, thereby making recovery more difficult for those afflicted. Large multicenter trials have established clinical variables with nonrheumatic atrial fibrillation that are independently associated with stroke (19). These variables are age older than 65 to 75 years, history of previous stroke, transient ischemic attack or peripheral thromboembolism, heart failure, systemic hypertension, and diabetes. Echocardiographic predictors, such as left atrial size and left ventricular hypertrophy, have also been reported to be risk factors (14).
Only gold members can continue reading. Log In or Register to continue