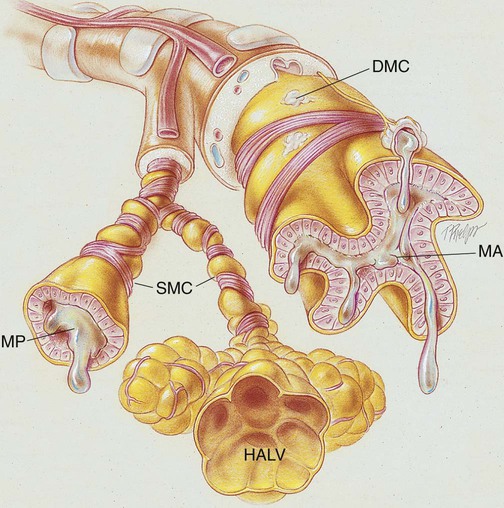
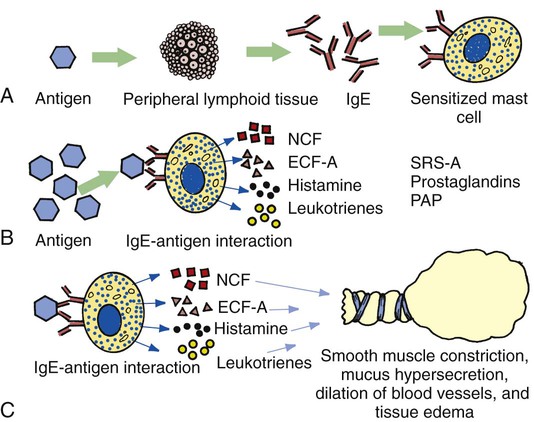
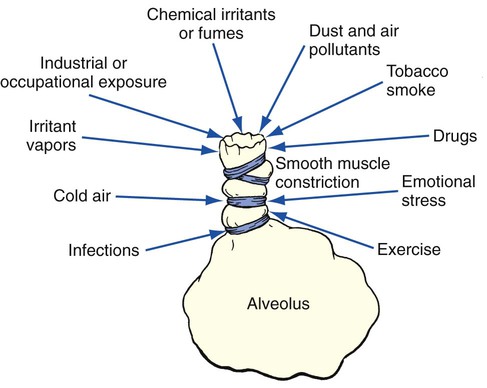
After reading this chapter, you will be able to: • Describe the role of the following organizations in the management of asthma: • National Asthma Education and Prevention Program (NAEPP) • Global Initiative for Asthma (GINA) • List the anatomic alterations of the lungs associated with asthma. • Describe the epidemiology and risk factors associated with asthma, including the following types of asthma: • Describe the challenges associated with the diagnosis of asthma, and include the tests used to diagnosis and monitor asthma. • Differentiate the classifications of asthma severity. • Describe the cardiopulmonary clinical manifestations associated with asthma. • Describe the general management of asthma. • Describe the clinical strategies and rationales of the SOAPs presented in the case study. • Define key terms and complete self-assessment questions at the end of the chapter and on Evolve. The burdens associated with asthma in the United States—and worldwide—are enormous. Although the precise annual numbers are not known, asthma is clearly linked to a multitude of lost school days, countless missed work days, numerous doctor visits, frequent hospital outpatient visits, and recurrent emergency department visits and hospitalizations. According to the Department of Health and Human Services’ Centers for Disease Control and Prevention, within the United States in 2005 more than 22 million people were diagnosed with asthma, more than 12 million people had experienced an asthma episode in the previous year, and nearly 4000 Americans died of asthma.* The World Health Organization (WHO) estimates that about 180,000 people worldwide die because of asthma each year. Clearly, asthma’s impact on health, quality of life, and the economy is substantial. The first evidence-based asthma guidelines were published in 1991 by NAEPP, under the coordination of the National Heart, Lung, and Blood Institute (NHLBI) of the National Institutes of Health (NIH). These guidelines were updated in 1997, 2002, and 2007.† Today the guidelines are structured around the following four components of care: (1) assessment and monitoring of asthma, (2) patient education, (3) control of factors contributing to asthma severity, and (4) the pharmacologic treatments. The NAEPP “stepwise asthma management charts” have been widely used and now specify optimal treatment for specific age groups 0 to 4 years, 5 to 11 years, and 12 years and older. GINA* was launched in 1993 in collaboration with the National Heart, Lung, and Blood Institute of NIH and WHO. GINA works with a network of asthma experts and researchers, health-care professionals, professional organizations, and public health-care officials from around the world. GINA gathers and disseminates asthma-related information while also ensuring that a system is in place to incorporate the results of scientific investigations into asthma care. GINA’s specific goals are the following: • Increase awareness of asthma and it public health consequences • Promote identification of reasons for the increased prevalence of asthma • Promote study of the association between asthma and the environment • Reduce asthma morbidity and mortality • Improve management of asthma • Improve availability and accessibility of effective asthma therapy Collectively, by using the evidence-based guidelines provided by NAEPP, along with the extensive information gathered worldwide from asthma experts and researchers, GINA now provides an outstanding—and user-friendly—evidence-based guideline program for the management of asthma. As of this writing, the GINA programs, which are freely available on the internet (www.ginasthma.org), include the following publications: • Global Strategy for Asthma Management and Prevention (2007). Scientific information and recommendations for asthma programs. • Pocket Guide for Asthma Management and Prevention (2006). Summary of patient care information for primary health-care professionals. • Pocket Guide for Asthma Management and Prevention in Children (2006). Summary of patient care information for pediatricians and other health-care professionals. • What You and Your Family Can Do About Asthma. An information booklet for patients and their families. Asthma is described as a lung disorder characterized by (1) reversible bronchial airway smooth muscle constriction, (2) airway inflammation, and (3) increased airway responsiveness to an assortment of stimuli. During an asthma attack, the smooth muscles surrounding the small airways constrict. Over time the smooth muscle layers hypertrophy and can increase to three times their normal thickness. The airway mucosa becomes infiltrated with eosinophils and other inflammatory cells, which in turn causes airway inflammation and mucosal edema. The goblet cells proliferate, and the bronchial mucous glands enlarge. The airways become filled with thick, whitish, tenacious mucus. Extensive mucous plugging and atelectasis may develop. The cilia are damaged, and the basement membrane of the mucosa is thicker than normal. As a result of smooth muscle constriction, bronchial mucosal edema, and excessive bronchial secretions, air trapping and alveolar hyperinflation develop. If chronic inflammation develops over time, these anatomic alterations become irreversible, resulting in loss of airway caliber. A remarkable feature of bronchial asthma, however, is that many of the pathologic anatomic alterations of the lungs that occur during an asthmatic attack are completely absent between asthmatic episodes (Figure 12-1). The major pathologic or structural changes observed during an asthmatic episode are as follows: 1. When a susceptible individual is exposed to a certain antigen, lymphoid tissue cells form specific IgE (reaginic) antibodies. The IgE antibodies attach themselves to the surface of mast cells in the bronchial walls (Figure 12-2, A). 2. Reexposure or continued exposure to the same antigen creates an antigen-antibody reaction on the surface of the mast cell, which in turn causes the mast cell to degranulate and release chemical mediators such as histamine, eosinophil chemotactic factor of anaphylaxis (ECF-A), neutrophil chemotactic factors (NCFs), leukotrienes (formerly known as slow-reacting substances of anaphylaxis [SRS-A]), prostaglandins, and platelet-activating factor ([PAP]; Figure 12-2, B). 3. The release of these chemical mediators stimulates parasympathetic nerve endings in the bronchial airways, leading to reflex bronchoconstriction and mucous hypersecretion. Moreover, these chemical mediators increase the permeability of capillaries, which results in the dilation of blood vessels and tissue edema (Figure 12-2, C). Occupational asthma is defined as asthma caused by exposure to an agent encountered in the work environment. More than 300 different substances have been associated with occupational asthma. Occupational asthma is seen predominantly in adults. It is estimated that occupational sensitizers cause about 1 in 10 cases of asthma among adults of working age. High-risk work environments for occupational asthma include farming and agricultural work, painting (including spray painting), cleaning work, and plastic manufacturing. Most occupational asthma is immunologically mediated and has a latency period of months to years after the onset of exposure. Although the cause is not fully understood, it is known that an IgE-mediated allergic reaction and cell-mediated allergic reactions are often involved. Box 12-1 shows additional agents known to cause occupational asthma. When an asthmatic episode cannot be directly linked to a specific antigen or extrinsic inciting factor, it is referred to as intrinsic asthma (also called nonallergic or nonatopic asthma) (Figure 12-3). The etiologic factors responsible for intrinsic asthma are elusive. Individuals with intrinsic asthma are not hypersensitive or atopic to environmental antigens and have a normal serum IgE level. The onset of intrinsic asthma usually occurs after the age of 40 years, and typically there is no strong family history of allergy. Furthermore, the diagnosis of asthma is often missed in the patient who acquires asthma in the workplace. This form of asthma is called occupational asthma (see Box 12-1). Because occupational asthma usually has a slow and insidious onset, the patient’s asthma is often misdiagnosed as chronic bronchitis or COPD. As a result, the asthma is either not treated at all or treated inappropriately. Finally, even though asthma can usually be distinguished from COPD, in some patients—those who have chronic respiratory clinical manifestations and fixed airflow limitations—it is often very difficult to differentiate between the two disorders—that is, asthma or COPD. These symptoms often respond to appropriate antiasthma therapy.
Asthma
Introduction
National Asthma Education and Prevention Program
Global Initiative for Asthma
Anatomic Alterations of the Lungs
Etiology and Epidemiology
Risk Factors
Extrinsic Asthma (Allergic or Atopic Asthma)
Immunologic mechanism
Occupational sensitizers (occupational asthma)
Intrinsic Asthma (Nonallergic or Nonatopic Asthma)
Diagnosis of Asthma
Diagnostic and Monitoring Test for Asthma
Asthma