Asthma
Marie-Christine Aubry, M.D.
Allen P. Burke, M.D.
Incidence
Asthma has a high prevalence, affecting 6% to 10% of the US population. Although present in all age groups, the prevalence of asthma is higher in children. Women and blacks are also more likely to develop asthma over the course of their life.1 Allergic diseases, such as asthma, have markedly increased in the past half century and are associated with urbanization.2
Clinical
Asthma almost always starts in childhood, upon sensitization to common inhaled allergens, such as house dust mites, cockroaches, animal dander, fungi, and pollens. In addition to atopy, other potential risk factors include secondhand exposure to smoking, respiratory infections, obesity, and some occupations. Clinically, asthma may present as sudden onset of bronchoconstriction and wheezing that may be life-threatening “asthma attacks,” or have a more indolent course. Patients may complain of cough, tightness of chest, and breathlessness, and these symptoms characteristically are variable and triggered by factors such as exercise, infection, allergens, and drugs. Other clinical conditions are seen in patients with asthma and may cause exacerbation of their asthma. These include eosinophilic pneumonia (Chapter 26), eosinophilic granulomatosis with polyangiitis (aka Churg-Strauss syndrome) (Chapter 49), rhinosinusitis, and allergic bronchopulmonary aspergillosis (Chapter 33). Although there may be some overlap in airway obstruction and reversibility with chronic obstructive pulmonary diseases, these two conditions are considered separate clinically. The diagnosis of asthma is based on a compatible clinical history, spirometry confirming response to bronchodilators, response to trial of steroids, and positive exercise test.
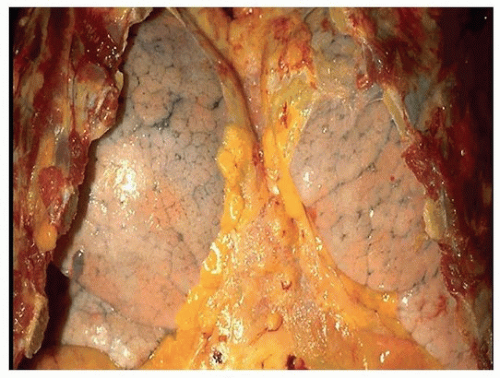 FIGURE 32.1 ▲ Autopsy lungs, patient dying from acute asthma attack “status asthmaticus.” The lungs are hyperinflated, such that they nearly approach at midline after removal of the chest wall. |
Pathophysiology
The hallmarks of asthma are reversible airflow obstruction, nonspecific bronchial hyperreactivity, and chronic airway inflammation. Dendritic cells take up allergens, process antigens, and present them to naive helper T cells, resulting in the activation of allergen-specific Th2 cells. Also involved are Th17 and Th9 T lymphocytes, which produce IL-17A, IL-17F, and IL-22, inducing airway inflammation and smooth muscle contraction.
Radiologic Findings
During an attack, chest x-rays may show hyperinflation, bronchial thickening, and focal atelectasis, or be completely normal. Complications such as consolidation and pneumomediastinum can also been seen on chest x-ray.3
High-resolution computed tomography is useful in patients with chronic or recurring symptoms to exclude possible associated disease such as allergic bronchopulmonary aspergillosis (see Chapter 33) and bronchiectasis (see Chapter 31). Expiratory scans are useful in demonstrating a mosaic pattern of lung attenuation with lucent areas representing air trapping.
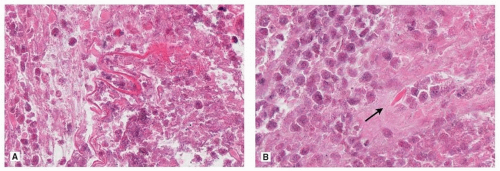 FIGURE 32.2 ▲ A. Curschmann spiral. The spiral is an elongated, serpiginous mucus strand. B. Charcot-Leyden crystal (arrow). Rhomboid-shaped crystal in a background of necrotic eosinophils. |



