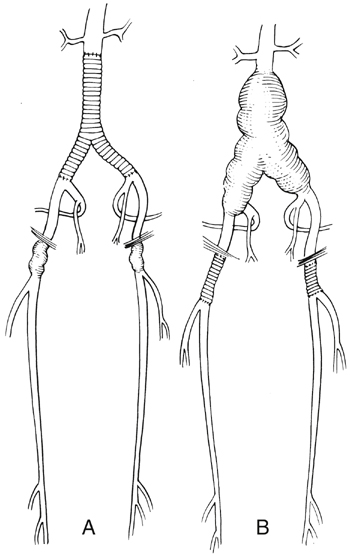
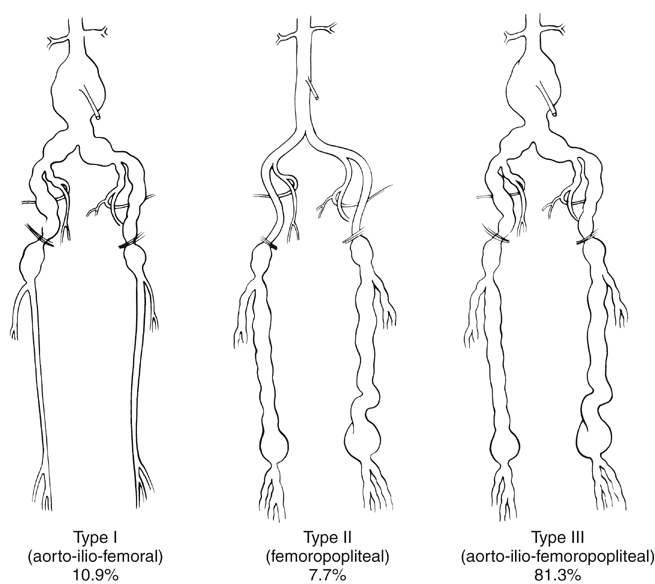
Arteriomegaly with aneurysms or aneurysmosis can be classified into three types based on the location and degree of arterial involvement. This classification, based on a review of 5771 aortofemoral angiograms performed at the Mayo Clinic from 1986 to 1982, revealed 300 patients with radiographic findings of arteriomegaly, including 91 (30.3%) with diffuse aneurysmal involvement or aneurysmosis (Figure 1). Femoral involvement can be treated with an appropriate interposition graft. In cases with involvement of the external iliac and/or hypogastric artery, the distal anastomosis is performed to the bifurcation of the distal common femoral artery. Reimplantation of at least one hypogastric artery should be included with the repair, and proximal aneurysmal degeneration can be treated with a short interposition graft (Figures 2 and 3). The presence of a large or obviously patent inferior mesenteric artery, on which the sigmoid colon blood supply depends, is an indication that the inferior mesenteric artery might need to be reimplanted into the main body of the graft.
Arteriomegaly and Aneurysmosis
Classification
Surgical Management
Type I
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Arteriomegaly and Aneurysmosis