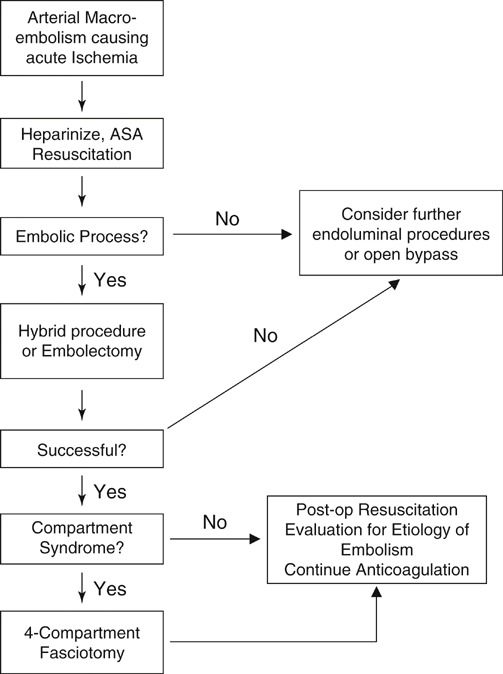
Choosing the appropriate therapy is also an important factor to decrease amputation occurrence and mortality (Figure 1). Although strong evidence suggests equivalence of endovascular or open surgical therapies, in terms of mortality and amputation, the etiology of the ALI needs to be factored into this equation.
Arterial Macroembolism
Diagnosis and Anatomy
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Thoracic Key
Fastest Thoracic Insight Engine