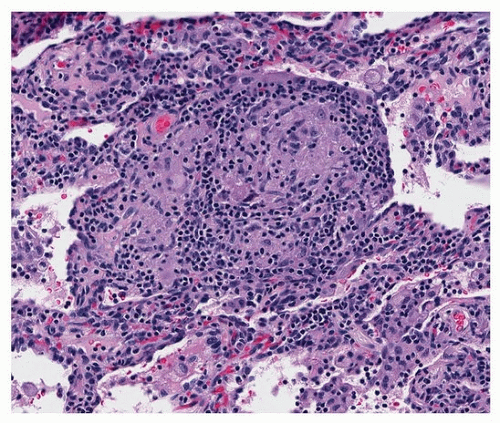
 FIGURE 9.1 ▲ Poorly formed granuloma. The interstitium contains chronic inflammation with granulomatous inflammation in the center (epithelioid macrophages with a few giant cells). |
be mistaken for pneumoconiosis (Fig. 9.3). Asteroid bodies are also nonspecific features of well-formed granulomas (Fig. 9.4).
TABLE 9.1 Histologic Features of Pulmonary Granulomas | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


