Figure 16.1
Concept of ‘classic (conventional)’ segmental resection (segmentectomy). According to the classic (conventional) concept of segmental resection, the segmental artery and bronchus, which run parallel, are both divided at the pulmonary hilum, while the intersegmental vein, which runs on the intersegmental plane, is carefully preserved only by cutting the branches to the resected segment
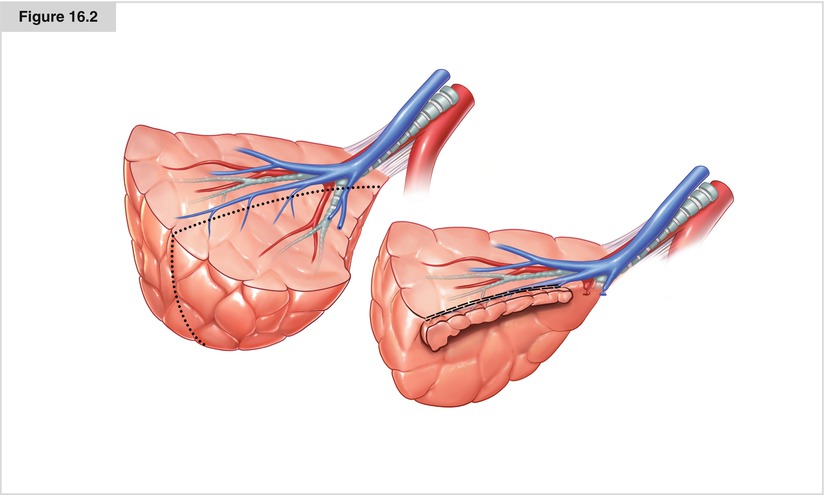
Figure 16.2
Concept of “modified (easy)” segmental resection (segmentectomy). In the modified concept of segmental resection, the entire segmental artery, vein, and bronchus are divided at the hilum. In this case, it is not necessary to expose the intersegmental vein on the intersegmental plane; therefore, it becomes easier to maneuver with staplers in dividing the intersegmental parenchyma. This modified technique may be justified not only because of the easy maneuverability but also because of the anatomic considerations with regard to the lymphatics in the lung parenchyma, especially in malignant cases
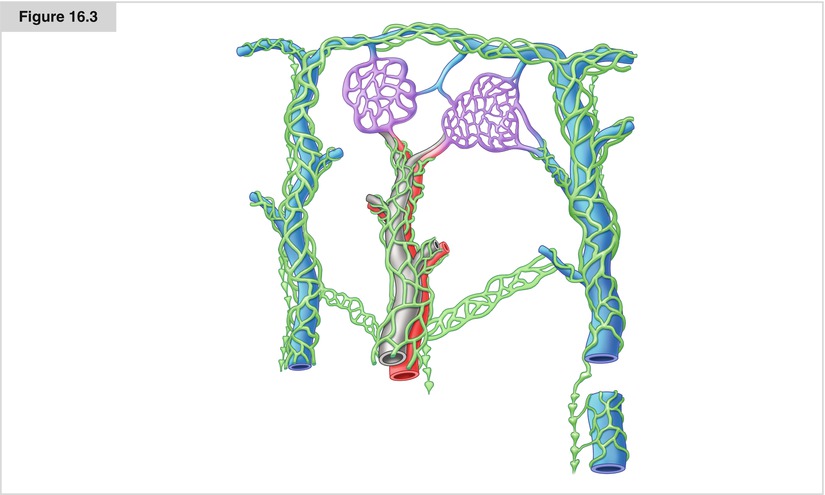
Figure 16.3
Network of lymphatics around the intersegmental vein and beneath the pleura. Surgeons who perform segmental resection should be familiar with the anatomy of lymphatics in the lung, because these are one of the main routes for the drainage of malignant cells to develop into lymph node metastases. In performing lobectomy, surgeons are not concerned about the intrapulmonary lymphatics, because these systems are resected en block together with the tumor-bearing lobe. However, in dissecting the lung parenchyma between neighboring segments, surgeons should be aware of the dense network of lymphatics around the intersegmental vein. To preserve these veins essentially means to preserve the lymphatics, which might possibly contain malignant cells, as well. Therefore, a careful and prudent approach might be required to preserve the intersegmental vein
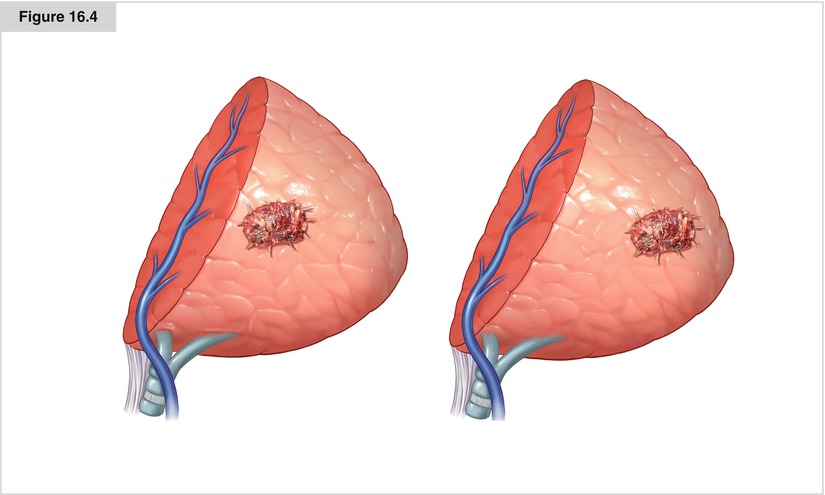
Figure 16.4
Factors closely related to local recurrence in segmental resection. How to divide the intersegmental lung parenchyma is another debate with regard to the technical aspects of segmental resections. Although any one of the methods—such as finger fracturing, electrocautery, or stapling—may be chosen, surgeons should be concerned about the tumor–surgical margin distance in relation to the local recurrence. Local recurrence on the segmental plane is most influenced by distance, not by the method for dividing the intersegmental parenchyma
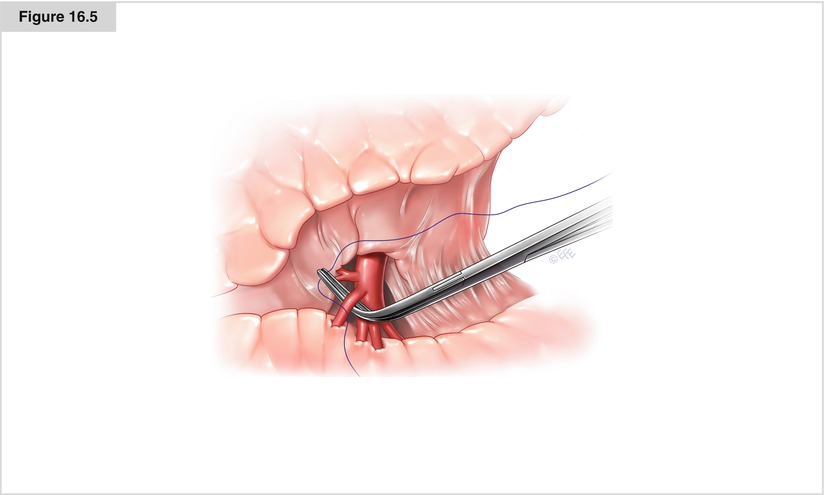
Figure 16.5




Ligation of the superior segmental artery. There have been several variations in the technical aspects of segmentectomy, especially with regard to the method for transecting the lung parenchyma on the intersegmental plane (finger fracture versus electrocautery versus stapling) and for preserving the intersegmental pulmonary vein. In the conventional technique, the principle of segmentectomy includes parenchymal dissection that exposes the veins in the intersegmental plane and division of its branches coming from the resected segment. However, in the presence of dense lymphatic networks along with intersegmental veins, which might be a drainage route for malignant cells, preserving the intersegmental vein might not be desirable in terms of curability. Presently, the most popular approach to segmental resection is the standard lateral thoracotomy position using general anesthesia with the ability to provide single-lung ventilation. There is not much difference between the procedure for superior segmentectomy on the left side and that on the right; the right-sided procedure is described here. The first step of this procedure is accessing the pulmonary artery through the major fissure between the upper and lower lobes, followed by division of the segmental artery, bronchus, and vein, and transection on the intersegmental plane. The technique for reaching the intermediate pulmonary artery trunk between the upper and lower lobes in segmentectomy is essentially the same as the one for lobectomy. Usually, the intermediate pulmonary artery trunk is accessed directly by dividing the visceral pleura and underlying parenchyma. The anatomy of the intermediate pulmonary artery trunk is then carefully inspected to confirm the branching of the segmental arteries. Rarely, the branches to the superior segment (lower lobe) and posterior segment (upper lobe) share a common trunk, whereas two separate branches to the superior segment originate from the intermediate trunk. The segmental branch is carefully tied and divided
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
