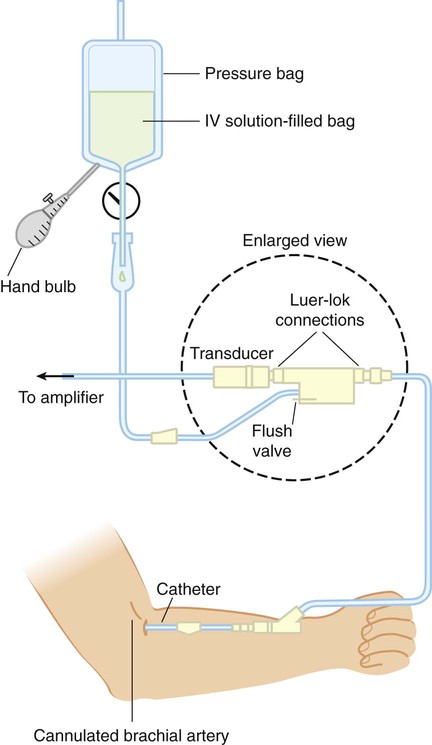
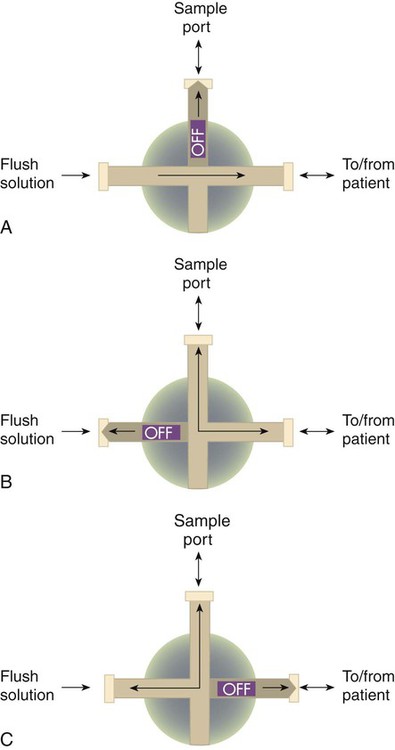
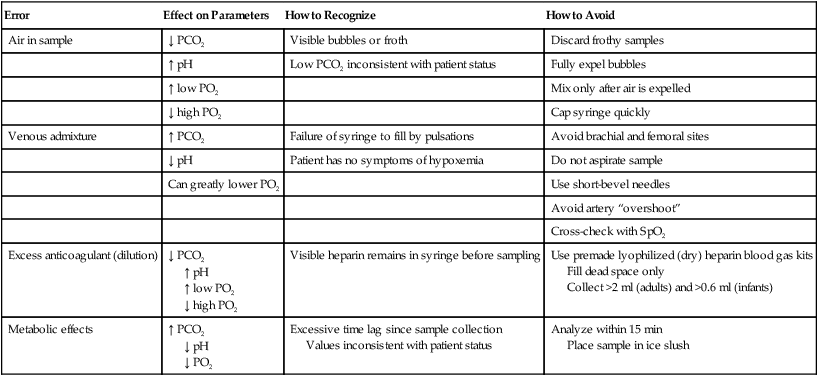
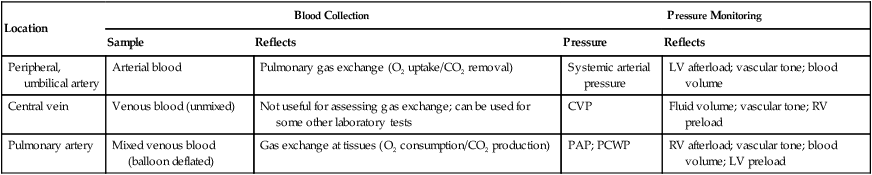
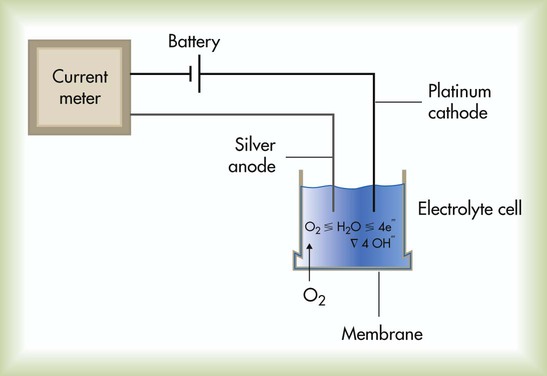
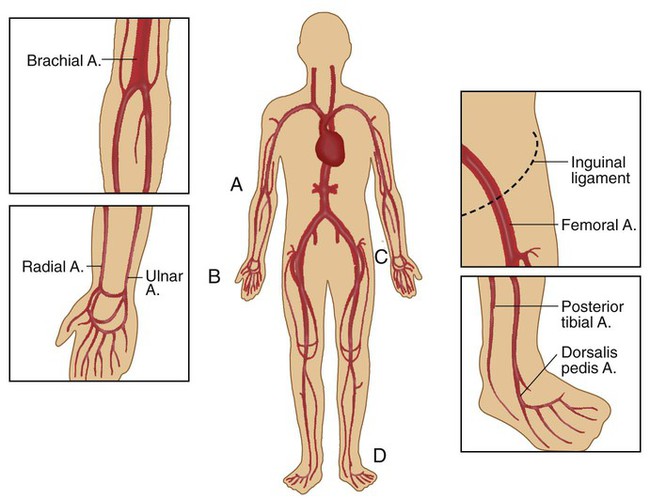
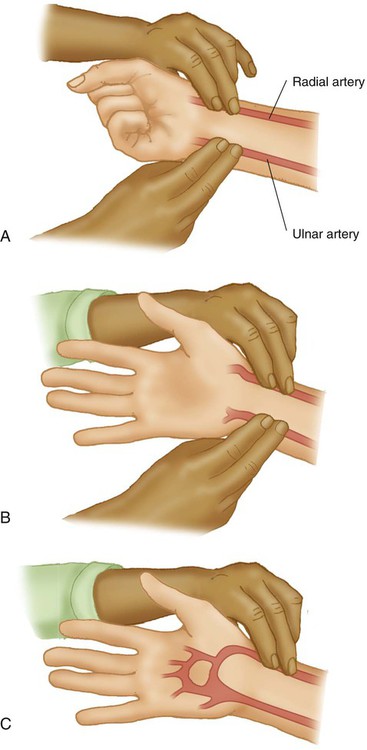
After reading this chapter you will be able to: Invasive procedures require insertion of a sensor or collection device into the body, whereas noninvasive monitoring is a means of gathering data externally.1 Because laboratory analysis of gas exchange requires blood samples, it is usually considered invasive. Monitoring can be either invasive or noninvasive. Generally, invasive procedures tend to provide more accurate data than noninvasive methods, but they carry greater risk. Although many methods exist for measuring O2 concentrations, most bedside systems apply electrochemical principles. There are two common types of electrochemical O2 analyzers: (1) the polarographic (Clark) electrode and (2) the galvanic fuel cell. Under ideal conditions of temperature, pressure, and relative humidity, both types are accurate to within ± 2% of the actual concentration.1 The Clark electrode is similar to electrodes used in blood gas analyzers and transcutaneous monitors (see later section on Transcutaneous Blood Gas Monitoring). This system typically consists of a platinum cathode and a silver–silver chloride anode (Figure 18-1). O2 molecules diffuse through the sensor membrane into the electrolyte, where a polarizing voltage causes electron flow between the anode and cathode. While silver is oxidized at the anode, the flow of electrons reduces O2 (and water) to hydroxyl ions (OH−) at the cathode. The more O2 molecules that are reduced, the greater is the electron flow across the poles (current). The resulting change in current is proportional to the PO2, with its value displayed on a galvanometer, calibrated in percent O2. Response times for Clark electrode O2 analyzers range from 10 to 30 seconds. Clinicians have been using blood samples to assess gas exchange parameters for more than 50 years.2 The definition of respiratory failure still is based largely on blood gas measurements. Depending on the need, blood gas samples can be obtained by percutaneous puncture of a peripheral artery, from an indwelling catheter (arterial, central venous, or PA), or by capillary sampling. Arterial puncture involves drawing blood from a peripheral artery (radial, brachial, femoral, or dorsalis pedis) through a single percutaneous needle puncture (Figure 18-2). The radial artery is the preferred site for arterial blood sampling for the following reasons: • It is near the surface and relatively easy to palpate and stabilize. • Effective collateral circulation normally exists in the ulnar artery. • The artery is not near any large veins. To guide practitioners in providing quality care, the American Association for Respiratory Care (AARC) has published Clinical Practice Guideline: Sampling for Arterial Blood Gas Analysis.3 Complementary recommendations have been published by the National Committee for Clinical Laboratory Standards.4 Modified excerpts from the AARC guideline appear in Clinical Practice Guideline 18-1. Box 18-1 lists the equipment needed to perform an arterial puncture. Commercial vendors provide kits containing most of the equipment listed. If provided, the needle capping device serves two purposes. First, it isolates the sample from air exposure (to ensure accurate results). Second, it helps prevent inadvertent needlestick injuries. There are many different capping device designs; devices that allow single-handed recapping are preferred. If a capping safety device is not provided, the clinician should use the single-handed “scoop” method to cap the needle before removing it and plugging the syringe. Box 18-2 outlines the basic procedure for radial artery puncture of adults. Before radial artery puncture is performed, a modified Allen test (Figure 18-3) is recommended. The test is normal (indicating adequate collateral circulation) if the palm, fingers, and thumb flush pink within 5 to 10 seconds after pressure on the ulnar artery is released. A normal test result indicates the presence of collateral circulation but may not predict the development of complications after radial artery puncture or cannulation. The modified Allen test has been a widely used clinical method to assess adequacy of ulnar artery collateral blood flow despite the lack of evidence that it can predict ischemic complications in the setting of complete radial artery occlusion.5 The criteria for an abnormal test result are not agreed on, which renders the significance of an abnormal test unclear. The test result may be inaccurate in predicting postcannulation hand ischemia, has poor interrater reliability, and is known to yield a high incidence of false normal and abnormal results. The modified Allen test cannot be performed on most critically ill patients who are either uncooperative or unconscious. In addition, prior radial artery cannulation, severe circulatory insufficiency, wrist or hand burns, or jaundice makes interpreting the results difficult. Performance of a modified Allen test before radial artery puncture or cannulation should not be considered a “standard of care,” but the need for its use and appropriate application should be well recognized.6 In patients who have undergone previous radial artery cannulation, the modified Allen test can provide documentation of possible arterial thrombosis and should be used to direct catheter placement. In that circumstance, it is imprudent to ignore totally the utility of the modified Allen test, especially if another arterial site is available for cannulation.7 • Never recap a used needle without a safety device; never handle a used needle using both hands; never point a used needle toward any part of the body. • Never bend, break, or remove used needles from syringes by hand. • Always dispose of used syringes, needles, and other sharp items in appropriate puncture-resistant sharps containers. Knowing when to obtain a blood gas sample is just as important as knowing how to perform the procedure. See Clinical Practice Guideline 18-1 for the general indications for ABG sampling. Box 18-3 lists common clinical situations associated with the need for ABG analysis. Preanalytic errors are problems occurring before sample analysis that can alter the accuracy of the blood gas results. Table 18-1 summarizes the most common errors associated with arterial blood sampling, including recommendations on how to recognize and avoid these problems.8,9 Clinicians can avoid most preanalytic errors by ensuring that the sample is obtained anaerobically, is properly anticoagulated (with immediate expulsion of air bubbles), and is analyzed within 10 to 30 minutes. TABLE 18-1 Preanalytic Errors Associated With Arterial Blood The traditional method used to avoid preanalytic errors caused by blood cell metabolism is to chill the sample quickly by placing it in an ice slush. Chilling is needed if the sample is not to be analyzed within 10 to 30 minutes.3 Chilled samples should be discarded if they are not analyzed within 60 minutes. PaO2 of samples drawn from subjects with elevated white blood cell counts may decrease rapidly, and immediate chilling is recommended. Chilled samples can result in potassium transport between blood cells and plasma and can result in erroneous elevation in potassium measured from a blood gas sample. Use of a glass syringe or a plastic syringe with low diffusibility minimizes the risk of room air gases contaminating the sample. Pneumatic tube transport of samples containing small air bubbles can have a noticeable effect on increasing PaO2.9 SaO2 represents the degree to which the hemoglobin (Hb) is saturated with O2 (see Chapter 11). Normally, the Hb saturation with O2 is 95% to 100% with healthy lungs. When the lungs cannot transfer O2 into the blood at normal levels, the SaO2 decreases in most cases in proportion to the degree of lung disease present. Blood gas analyzers report a calculated SaO2. Measurement of SaO2 by hemoximetry and Hb content is required for accurate determination of CaO2. The acid-base status of the patient is determined by evaluating the pH, PaCO2, and plasma HCO3−. The steps for interpreting the acid-base status of the ABG results are described in Chapter 13. The most common routes for indwelling vascular lines are a peripheral artery (usually radial, brachial, or less commonly dorsalis pedis and axillary) or femoral artery, a central vein (usually the vena cava), and the PA. In neonates, the umbilical artery is cannulated for arterial blood sampling. Table 18-2 summarizes the usefulness of these various sites in providing relevant clinical information. Chapter 46 provides details on the use of these systems for hemodynamic pressure and flow monitoring. TABLE 18-2 Common Sites for Indwelling Vascular Catheters and the Information They Provide Figure 18-4 shows the basic setup used for an indwelling vascular line, in this case, a brachial artery catheter. The catheter connects to a disposable continuous-flush device (Delta-flow; Utah Medical Products, Midvale, UT). This device keeps the line open by providing a continuous low rate of flow (2 to 4 ml/hr) of intravenous saline solution through the system. Heparinized saline flush solution has been commonly used with indwelling vascular catheters. However, it has been shown that heparin does not significantly improve arterial catheter function, extend the duration of use, or decrease the number of manipulations required. Additionally, results of coagulation studies can be affected by heparinized flush solution, and unnecessary exposure to heparin may increase the risk of heparin-induced thrombocytopenia.10 Because arterial pressures are much higher than venous pressures, the intravenous bag supplying these systems must be pressurized, usually by using a hand bulb pump. A strain-gauge pressure transducer connected to the flush device provides an electrical signal to an amplifier or monitor, which displays the corresponding pressure waveform. Access for sampling blood from most intravascular lines is provided by a three-way stopcock (Figure 18-5). Equipment and supplies are the same as specified for arterial puncture, with the addition of a second “waste” syringe. Box 18-4 outlines the proper procedure for taking an arterial blood sample from a three-way stopcock system. With the exception of venous admixture, the preanalytic errors that occur when sampling blood from a vascular line are the same as the errors that occur with intermittent puncture, as are the ways to avoid them. For clinicians, the challenge with vascular lines is to maintain their function properly and troubleshoot the many potential problems that can occur. Because these are key components of bedside monitoring skills, they are discussed in the section on hemodynamics in Chapter 46. Capillary blood gas sampling is used as an alternative to direct arterial access in infants and small children. Properly obtained capillary blood from a well-perfused patient can accurately reflect and provide clinically useful estimates of arterial pH and PCO2 levels.6 However, capillary PO2 is of no value in estimating arterial oxygenation, and O2 saturation by pulse oximetry must also be evaluated when a capillary blood gas sample is obtained. Respiratory therapists (RTs) must exercise extreme caution when using capillary blood gases to guide clinical decisions. Direct arterial access is still the preferred approach for assessing gas exchange in infants and small children with severe acute respiratory failure. Capillary blood values are meaningful only if the sample site is properly warmed. Warming the skin (to approximately 42° C) causes dilation of the underlying blood vessels, which increases capillary flow well above tissue needs. Blood gas values resemble the values in the arterial circulation; this is why a sample obtained from a warmed capillary site is often referred to as arterialized blood. It has been shown that capillary blood samples from the earlobe reflect arterial PCO2 and PO2 better than samples drawn from a finger stick.11 The posterior medial or lateral curvature of the heel is the recommended site for capillary puncture specimens in infants less than 1 month old to avoid nerve and bone damage. To guide practitioners in providing quality care, the AARC has published Clinical Practice Guideline: Capillary Blood Gas Sampling for Neonatal and Pediatric Patients.12 Modified excerpts from the AARC guideline appear in Clinical Practice Guideline 18-2. Sampling of capillary blood is useful for patient management only if the procedure is performed according to an established quality assurance program. The most common technical errors in capillary sampling are inadequate warming of the capillary bed and squeezing of the puncture site. Squeezing the puncture site may result in venous and lymphatic contamination of the sample.13
Analysis and Monitoring of Gas Exchange
 Describe the difference between monitoring and analysis.
Describe the difference between monitoring and analysis.
 Describe the two types of electrochemical oxygen analyzers.
Describe the two types of electrochemical oxygen analyzers.
 Describe calibration and problem-solving techniques for oxygen analyzers.
Describe calibration and problem-solving techniques for oxygen analyzers.
 State how to obtain, process, and analyze arterial and capillary blood gas samples.
State how to obtain, process, and analyze arterial and capillary blood gas samples.
 List the quality control procedures applied to blood gas analysis.
List the quality control procedures applied to blood gas analysis.
 List the potential advantages of point-of-care testing.
List the potential advantages of point-of-care testing.
 Describe how to obtain and interpret transcutaneous oxygen and carbon dioxide monitoring.
Describe how to obtain and interpret transcutaneous oxygen and carbon dioxide monitoring.
 Describe the basic principles used by an oximeter to monitor oxygen saturation.
Describe the basic principles used by an oximeter to monitor oxygen saturation.
 State when and how to perform pulse oximetry.
State when and how to perform pulse oximetry.
 Identify true statements related to interpretation of pulse oximetry results.
Identify true statements related to interpretation of pulse oximetry results.
 Describe how to perform capnometry and interpret capnograms.
Describe how to perform capnometry and interpret capnograms.
Invasive Versus Noninvasive Procedures
Measuring Fractional Inspired Oxygen
Instrumentation
Sampling and Analyzing Blood Gases
Sampling
Arterial Puncture and Interpretation
Equipment
Procedure
Indications for Blood Gas Sampling
Problem Solving and Troubleshooting
Preanalytic Error
Error
Effect on Parameters
How to Recognize
How to Avoid
Air in sample
↓ PCO2
Visible bubbles or froth
Discard frothy samples
↑ pH
Low PCO2 inconsistent with patient status
Fully expel bubbles
↑ low PO2
Mix only after air is expelled
↓ high PO2
Cap syringe quickly
Venous admixture
↑ PCO2
Failure of syringe to fill by pulsations
Avoid brachial and femoral sites
↓ pH
Patient has no symptoms of hypoxemia
Do not aspirate sample
Can greatly lower PO2
Use short-bevel needles
Avoid artery “overshoot”
Cross-check with SpO2
Excess anticoagulant (dilution)
↓ PCO2
↑ pH
↑ low PO2
↓ high PO2
Visible heparin remains in syringe before sampling
Use premade lyophilized (dry) heparin blood gas kits
Fill dead space only
Collect >2 ml (adults) and >0.6 ml (infants)
Metabolic effects
↑ PCO2
↓ pH
↓ PO2
Excessive time lag since sample collection
Values inconsistent with patient status
Analyze within 15 min
Place sample in ice slush
Interpretation of Arterial Blood Gases
Indwelling Catheters (Arterial and Central Venous Pressure and Pulmonary Artery Lines)
Location
Blood Collection
Pressure Monitoring
Sample
Reflects
Pressure
Reflects
Peripheral, umbilical artery
Arterial blood
Pulmonary gas exchange (O2 uptake/CO2 removal)
Systemic arterial pressure
LV afterload; vascular tone; blood volume
Central vein
Venous blood (unmixed)
Not useful for assessing gas exchange; can be used for some other laboratory tests
CVP
Fluid volume; vascular tone; RV preload
Pulmonary artery
Mixed venous blood (balloon deflated)
Gas exchange at tissues (O2 consumption/CO2 production)
PAP; PCWP
RV afterload; vascular tone; blood volume; LV preload
Equipment
Procedure
Problem Solving and Troubleshooting
Capillary Blood Gases
Problem Solving and Troubleshooting
Analysis and Monitoring of Gas Exchange
 Rule of Thumb
Rule of Thumb