Infectious diseases
Invasive aspergillosis
Chronic necrotising pulmonary aspergillosis/Aspergilloma
Hypersensitivity diseases
Aspergillus sensitisation in asthma
And severe asthma associated with fungal sensitization (SAFS)
Hypersensitivity pneumonitis
Allergic bronchopulmonary aspergillosis
Aspergillus: An Ubiquitous Fungus
Aspergillus organisms are filamentous fungi and are extremely resilient. AF is ubiquitous in the environment, in water, soil spaces, wood chips, grass mowings, potted plants, indoor air, walls and ceilings, building demolitions, etc… The spores are capable of withstanding extreme atmospheric conditions, grow at temperatures ranging from 15 to 50 °C and survive even at >55 °C [9, 26]. Inhalation of spores (conidia) from the environment is followed by growth of hyphae in the mucus of the bronchial tree. AF germination is the transformation from conidia to hyphae. In its mycelium phase, AF consists of 7–10 μm long, uniform, septate hyphae with dichotomus branching at an angle of 45°. The hyphae can be identified using the PAS and Grocott’s stains. Reproduction is characterised by the formation of conidiophores with terminal vesicles producing chains of spores. The spores measure 2–4 mm in diameter. AF grows on Sabouraud dextrose agar slants [27]. It takes about 12 h for AF to germinate at 37 °C on simple media and 4–5 h on rich media. Conidiophores and spores may be seen together, mainly in structures that are in contact with the atmosphere.
The relationship between ABPA development and level of AF exposure remains unclear, even if high levels of AF exposure have been associated with ABPA exacerbation and if the prevalence of ABPA varies according to climate [28].
Pathogenesis: From AF Spore Inhalation to ABPA
Factors underlying the development of ABPA remain unclear. Up to 25 % of asthmatics are sensitised to AF [29] and multiple sensitisations to fungi should be associated with more severe asthma [30]. Yet, few asthmatics develop an ABPA. ABPA mainly occurs in atopic patients. The bronchopulmonary response to inhalation of Aspergillus spores involves three associated factors: fungal proliferation, hypersensitivity and abnormalities of the bronchial epithelium (Fig. 5.1). After A. fumigatus spores are inhaled into the bronchial airways, they are usually trapped by the luminal mucus and then destroyed by mechanisms of local defence. However, proliferation of A. fumigatus with mycelia formation can occur if there are abnormalities in the immune response (local defence with development of an aspergilloma inside a residual cavity devoid of alveolar macrophages and neutrophils, or in COPD patients; systemic defence in cases of invasive aspergillosis). The second response mechanism is hypersensitivity likely to induce either an IgG response with complement activation (rare cases of hypersensitivity pneumonitis) or, in atopic patients, an IgE response consecutive to sensitisation to A. fumigatus (allergic asthma). ABPA is different and is characterised by markedly elevated Aspergillus-specific IgE, IgA and total IgE antibodies, eosinophilic pulmonary infiltrates, bronchiectasis and fibrosis. Several associated concomitant factors favour ABPA development. Among these factors, the respective roles of genetics and pre-activation of epithelial cells (and the extent to which this activation facilitates bronchial penetration of the fungus) as well as the immune response (bronchial/bronchiolar inflammation, remodelling and bronchial destruction) are not yet fully understood. Indeed, mechanisms involved in ABPA development are complex (Fig. 5.1). Pepys suggested that ABPA was the result of type I and type III immunologic responses, classified according to Gell and Coombs. However, this classification probably provides an excessively restricted view of ABPA pathogenesis.
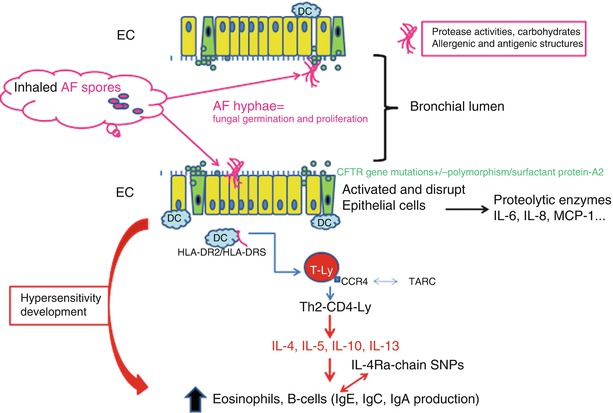
Fig. 5.1
Pathophysiology of ABPA. AF spores germinate in a predisposing environment. AF products (hyphae++  ) disrupt epithelial junctions and activate epithelial cells (EC)-secreting proteolytic factors and pro-inflammatory mediators. Genetic factors (implicated in surfactant production, CFTR gene) may limit the host defence and encourage AF germination. Allergens are presented by the dendritic cells (DC)/macrophages (which preferentially express HLA-DR2 and 5) to T lymphocytes, with a predominant Th2 response. IL4Ra chain SNPs in ABPA may in part induce an IL-4 “hypersensitivity”. This results in the production of high levels of IgE and IgG
) disrupt epithelial junctions and activate epithelial cells (EC)-secreting proteolytic factors and pro-inflammatory mediators. Genetic factors (implicated in surfactant production, CFTR gene) may limit the host defence and encourage AF germination. Allergens are presented by the dendritic cells (DC)/macrophages (which preferentially express HLA-DR2 and 5) to T lymphocytes, with a predominant Th2 response. IL4Ra chain SNPs in ABPA may in part induce an IL-4 “hypersensitivity”. This results in the production of high levels of IgE and IgG
) disrupt epithelial junctions and activate epithelial cells (EC)-secreting proteolytic factors and pro-inflammatory mediators. Genetic factors (implicated in surfactant production, CFTR gene) may limit the host defence and encourage AF germination. Allergens are presented by the dendritic cells (DC)/macrophages (which preferentially express HLA-DR2 and 5) to T lymphocytes, with a predominant Th2 response. IL4Ra chain SNPs in ABPA may in part induce an IL-4 “hypersensitivity”. This results in the production of high levels of IgE and IgGA Main Role for Genetic Factors
CD4 + Th2 lymphocytes from ABPA patients are restricted to six MHC class II human leucocyte antigen (HLA)-DR subtypes. Genetic studies suggest that HLA-DR2 and HLA-DR5 are associated with susceptibility to ABPA, whereas HLA-DQ2 is associated with resistance [31–33]. Restricted genotypes within these HLA subtypes also influence the risk of ABPA. Chauhan et al. [31] has created an interesting hypothesis. He has shown that the affinity of Aspf1 for HLA-DR is low and that it may favour a Th2 cell response [31]. Indeed, T-cell receptor (TCR)-mediated signalling pathways can be modified by stimulating T cells using peptides with low affinity for a particular TCR [34]. It has been demonstrated in several model systems, in vivo and in vitro, that providing a weak TCR-mediated signal can preferentially generate IL-4-producing cells and Th2 differentiation. A strong HLA-DR-AgTCR affinity may tend to favour a Th1 cellular response, whereas low affinity favours a Th2 humoral response [35–37].
The combination of these data with mutations of the cystic fibrosis trans-membrane conductor regulator (CFTR) gene might determine the outcome of ABPA in patients with CF, but also in some asthmatics [38]. Marchand et al. found that the frequency of (CFTR) gene mutations was higher in non-CF patients with ABPA compared with allergic asthma, even though both groups showed normal sweat chloride concentrations [39]. Similar conclusions were made by Miller et al. [40]. This indicates that CFTR gene mutations are likely to participate in the development of ABPA, even if there are no data concerning the quality of mucus in these cases.
AF conidia bind surfactants A and D. Surfactant enhances phagocytosis of AF. Saxena et al. identified an association between two polymorphisms in the collagen region of pulmonary surfactant protein-A2 (ala91pro, arg94arg) and a predisposition to ABPA and severity of the disease [41]. About 80 % of patients carrying both alleles had ABPA, while 50 and 60 % carrying each allele had ABPA (p = 0.0079; OR: 10.4) [41].
A. fumigatus Mediators and/or Antigens: Actors of the Local Pro-inflammatory Response and the Specific Immune Response
A. fumigatus antigens have the capacity to interact with epithelial cells of the bronchial mucosa by releasing proteolytic enzymes that cause epithelial detachment and facilitate transport of antigens and allergens across the epithelial barrier. In addition, Tomee et al. [43] showed that human bronchial and alveolar epithelial cell lines produce large amounts of pro-inflammatory cytokines and chemokines (IL-6, IL-8 and monocyte chemotactic protein (MCP)-1) when incubated with A. fumigatus proteases, inducing additional epithelial activation. This activation process is partly dependent on protease-activated receptor 2 [44]. Moreover, the spectrum of response to recombinant A. fumigatus allergens suggests that some of them appear to be more strongly implicated in both Aspergillus sensitisation and ABPA [45]. Several proteases also have immunogenic properties [9]. Eosinophils are major cells causing inflammation in ABPA and eosinophil proteases and proteins may enhance epithelial destruction.
Induction of a Strong Th2-CD4+ T Cell Response, Characterised by a “Hypersensitivity to IL-4”
AF releases allergens during hypheal growth and more than 60 structures of AF are susceptible to bind IgE, and genetic analysis of Aspergillus species identified 30 allergens, including proteins, polysaccharides, glycoproteins, proteases (Aspf5, f10, f13, etc.…), glycosidases (Aspf2, 9…) and many proteins produced or secreted, some being involved in oxidative stress. ABPA occurs in immune-competent subjects and dysfunction or specific polymorphisms of genes encoding for the Toll-Like receptor (TLR)-2, 4 or 9 involved in recognition of specific AF motifs are not demonstrated in ABPA [21]. Allergens are processed by antigen-presenting cells and presented to T cells. ABPA is characterised by a strong Th2 CD4 response with two main consequences: the release of large amounts of IL-4 and IL-5 (and also IL-13), which explains the influx of eosinophils and hyper-IgE production namely during exacerbation episodes, as well as activation of B cells [46–50]. Lymphocyte activation has been shown in humans and in animal models [46–52]. In mice challenged with AF, there is an accumulation of pulmonary Th-2 cells with a higher number of granulocyte-macrophage colony-stimulating factor (GMCSF)-, IL-4- and IL-5-positive cells in the ABPA murine model than in controls [53], while IL-10 seems to act as a natural suppressor of the pro-inflammatory reaction [54, 55]. Nevertheless, regulating mechanisms are complex when there is an association between the −1082GG genotype of IL-10 promoter (increasing IL-10 synthesis) with AF colonisation and the development of ABPA in CF [56]. In patients with ABPA, peripheral blood mononuclear cells showed increased sensitivity to IL-4 [57]. IL-4 is involved in IgE production, but also eosinophil activation, via up regulation of very late antigen (VLA)-4 and C chemokine receptor (CCR)3 expression [57, 58]. Elevated blood sIL-2 receptor concentrations and higher levels of cluster differentiation (CD)23 expression on B cells were found in ABPA patients [59].
Compared with A. fumigatus-sensitised asthmatics without ABPA, the increase in CD23 expression is also partly mediated by IL-4 [60]. Recently, Hartl et al. [61] evaluated pro-Th2 chemokines in ABPA in patients with CF. Th2 cells preferentially expressed the chemokine receptor CCR4 and were attracted by the corresponding chemokines, thymus and activation-regulated chemokine (TARC) (CCL17) and macrophage-derived chemokines (MDC). The levels of TARC were elevated in ABPA when compared with atopic controls or CF without ABPA: these values increased significantly during acute exacerbations of ABPA, in parallel with total IgE levels. It is interesting to relate these data to the experimental study by Schuh et al. [62]: the CCR4 knock-out mouse model exhibited reduced bronchial hyper-responsiveness and more rapid clearance of AF, indicating a major role for CCR4 and TARC in the immune response to AF. Elevated serum TARC may be useful in CF patients for diagnosing ABPA [63]. TARC may link an antifungal immune response with the promotion of Th2 cells and hypersensitive response to AF [61].
Another indication of increased IL-4 sensitivity in ABPA was provided by Knutsen [64]: he studied the presence of IL-4 receptor α-chain single nucleotide polymorphisms (SNPs) in ABPA and showed that IL4R α chain SNPs were observed in 95 % of ABPA, with a predominance of extracellular IL-4R α SNP “ile75val”, present in 88 % of ABPA. The latter study suggested that this polymorphism might be a genetic marker of ABPA risk. Thus, IL-4 “hypersensitivity” is clearly involved in the amplified IgE response, and may play a major role in the B-cell hyper-reactivity in ABPA [37].
Amplification of the B-Cell Response
Amplification of the B-cell response: large amount of total serum IgE. The T-cell response in ABPA patients was associated with B-cell activation and the presence of large amounts of IgE, IgA and IgG in the blood and bronchial lumen [65]. Divergent results were obtained in studies of blood and bronchoalveolar lavage (BAL) fluids concerning the production of immunoglobulins directed against A. fumigatus. Such inconsistencies may be explained by differences in the detection methods used: some authors evaluated precipitating antibodies, whereas others used enzyme-linked immunosorbent assay (ELISA) or radio-immunoassay (RIA) methods. Moreover, the quality of antigen extracts differed considerably between studies. The use of recombinant antigens should improve detection rates and make the results of these studies more reproducible and reliable. The IgE response is largely, but not exclusively, directed towards A. fumigatus epitopes [66]. Indeed, mould AF contains abundant carbohydrates, including glycan, chitin and galactomannan. In mice sensitised with AF extracts treated by sodium-periodate that destroys carbohydrates, a significant decrease in both total and specific IgE was obtained, as well as a reduction in eosinophil recruitment. Indeed, carbohydrates present in ABPA play a key role as internal adjuvants in the total IgE response [67].
Tissue Damage
Tissue damage (bronchiectasis formation) occurs in ABPA patients as a consequence of the local influx of neutrophils and eosinophils. Sputum eosinophil and neutrophil counts are higher in ABPA patients with bronchiectasis than in those without bronchial destruction [68]. The extent of bronchiectasis, detected by high resolution computed tomography (CT) scan, correlates with the number of eosinophils and neutrophils in the sputum, but not with total IgE levels in the serum [68]. Recently, Gibson et al. demonstrated that IL-8 gene expression and IL-8 protein levels in the sputum were higher in ABPA patients than in controls, and the extent of these two parameters correlated with the degree of bronchial neutrophilia and airway obstruction [69]. Thus, IL8 may be a key mediator of tissue damage in ABPA.
Diagnosis
ABPA is defined by major diagnostic criteria – clinical, biological and radiological criteria – but definition remains debated and particularly difficult in CF patients (Tables 5.2 and 5.3) [9, 70–73].
Table 5.2
Diagnostic criteria for ABPA (not CF patients)
Table 5.3
Diagnostic criteria for ABPA in cystic fibrosis patients [9] (consensus conference recommendations for diagnosis for ABPA in CF). The classic diagnostic criteria for ABPA are in black text. The minimal diagnostic criteria for ABPA are written in red
Clinical Vignette
A 64 year old woman was referred to hospital for acute exacerbation of asthma.
Asthma was diagnosed at the age of 19 and “disappeared” during her 20s. At the age of 39, recurrence of asthmatic symptoms (coughing, wheezing, nocturnal symptoms) was observed. Since 6 years, asthma was controlled by formoterol and fluticasone (250 mg × 2/day), and salbutamol “as-needed”. Lung function tests performed 6 years-ago showed bronchial obstruction (a decrease FEV1 : 78 % of predicted value, with normal FVC : 98 % PV), which return to normal value after 1 month of inhaled treatment (FEV1: 92 % PV). The chest X-ray was normal. Skin prick tests showed sensitisations to Dermatophagoides pteronyssinus, cats, horses, Cladosporium sp. and Aspergillus fumigatus.
When admitted for acute exacerbation, the patient complained of frequent respiratory symptoms over the previous 8 months. She had required oral corticosteroids on six occasions in the previous 8 months, sometimes associated with antibiotics. She had dark sputum. Sometimes, she experienced right or left chest pain, increased by inspiration. She had no extra-respiratory manifestations.
On admission, the patient was febrile (39 °C), despite a treatment-associated amoxicilline-clavulanic acid and ciprofloxacin over the previous 72 h. She had not taken any oral steroids at that time. The chest auscultation showed crackles with reduced breath sounds in the left apical area and diffuse wheezing. She complained of left axillary chest pain. Sputum was purulent and brown.
Investigations showed:
An inflammatory syndrome: C-reactive protein: 67 mg/l
A blood eosinophilia (1,900 elements/mm3) and neutrophilia (8,200 elements/mm3)
Normal renal and liver laboratory tests
A high blood total IgE level (2,800 UI/ml)
No detection of blood anti-neutrophil cytoplasmic antibodies (ANCA)
Normal cardiac ultrasound was normal.
Upper left lobe atelectasia on the CT scan (Fig. 5.2a, b)
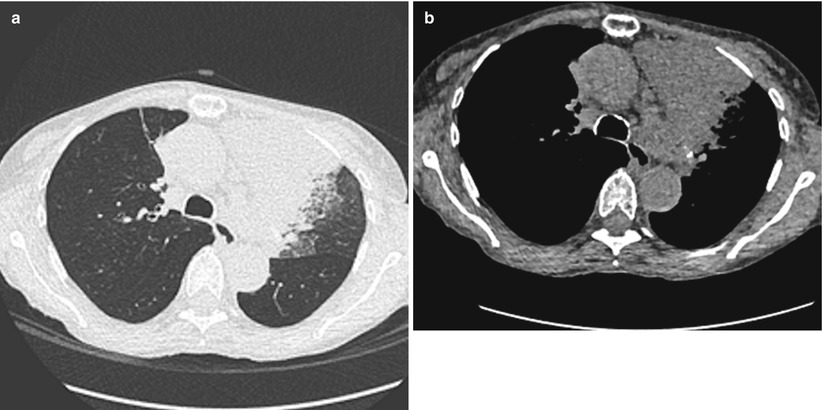
Fig. 5.2
(a) Parenchymental section and (b) mediastinal section: CT scan showing isolated upper left lobe atelectasia
No new sensitisations on the skin prick tests, compared with previous ones
Diagnosis of ABPA was presumed (asthma with “atypical symptoms”, pneumonia resistant to treatment, eosinophilia, elevated total IgE and no argument for a vasculitis).
Specific IgE assay against Aspergillus fumigatus antigen by Phadia CAP System (Kabi Pharmacia, Sweden) was positive (24 UI/mL).
An enzyme-linked immunosorbent assay for Aspergillus-specific IgG antibodies showed a titer of 3.98 indices.
An immunodiffusion precipitin test to detect Aspergillus-specific antibodies demonstrated a positive result (6 precipitin bands).
The patient was trea ted with steroids (0.5 mg/kg/day; e.g. 25 mg/day), physiotherapy and nebulisation of saline isotonic solution. After 4 days of treatment, the fever and the blood eosinophilia disappeared. FVC and FEV1 were respectively 68 % and 45 % of predicted values. The radiological aspect was not modified and flexible bronchoscopy was indicated. A voluminous mucus plug was obstructing the upper left bronchus, collecting multiple mucoid impactions after bronchio-alveolar lavage. AF hyphae were detected in BAL when other explorations were negative (bacterial and mycobacterial analysis).
After 7 days, the patient came out of hospital with a final diagnosis of sero-positive ABPA.
The detection of AF hyphae has led to treatment associated itraconazole (400 mg/day) and oral steroids (25 mg/day) for 2 weeks being proposed, then a slow decrease for a total period of 8 weeks). After 4 weeks, total IgE level was 740 UI/mL. She had no further sputum and chest pain. The inhaled treatment (fluticasone and formoterol association) was stopped.
The patient has been monitored in our institution for 6 years now and is still under itraconazole. When we tried to stop itraconazole on three occasions, a new exacerbation of ABPA occurred, with atelectasia or lung infiltrate, marked increase in total blood IgE, requiring high doses of steroids. Courses of steroids were prescribed seven times throughout these 6 years times. She still has blood total IgE ranging between 390 and 615 UI/mL.
The occurrence of asthma with frequent exacerbations, but with “atypical” symptoms of asthma led to discussion of an alternative diagnosis, particularly ABPA in this case.
Clinical Symptoms
The ABPA is more frequent in young adults between 30 and 40 years old. It can occur in childhood, but is less frequent during this period. In CF patients, it is recommended that the patient be tested for ABPA once a year after the age of 6 [9]. Most patients have atopic asthma and more than 60 % of CF patients with ABPA are atopic. ABPA may occur at the time of the asthma diagnosis or, more often, after the onset of asthma. Asthma symptoms may change with fever (body temperature reaching 38.5 °C), malaise, chest pain, thick, purulent, sometimes brown sputum. There may have cough, haemoptysis. Pulmonary consolidation without bacterial or viral infection has been observed. Physical examination does not add any information for ABPA diagnosis. Crackles are present at the stages of destruction. The diagnosis must be discussed in asthmatic patients with frequent exacerbations and/or requiring recurrent corticosteroid courses and/or hypereosinophilia. In refractory asthma, the diagnosis of ABPA must be challenged. In children, when ABPA is diagnosed, sweet chloride tests must be performed.
Radiological Patterns and Pulmonary Function Tests
Radiographic analyses (Figs. 5.3a, b and 5.4a, b) have been carried out on chest X-rays and high resolution CT (HRCT) scans. Some abnormalities tend to be transient, such as pulmonary infiltrates, the presence of fluid in the bronchi and lobar or segmental collapse linked to mucous plugs [72, 73]. Permanent patterns included bronchiectasis, most frequently in the upper lobes in the segmental and subsegmental bronchi, and cavities. HRCT scan was normal in 37 % of ABPA patients [74]. Bronchiectasis occurs at more central sites in ABPA patients than in those with other bronchial diseases. However, bronchiectasis has been reported in the peripheral airways in some ABPA cases [75, 76]. The presence of central bronchiectasis is not pathognomonic of ABPA and may have a low sensitivity, up to 37 % [76]. Analysis using plain film revealed that most patients (19/20; 95 %) had upper lobe abnormalities, but 9/20 had both upper and lower lobe involvement [77]. Descriptions of “glove-finger” opacities are common and correspond to bifurcating opacities caused by the bronchial distribution resulting from mucoid impaction. The collapse of a lobe segment, or an entire lobe, has been described and is often associated with clinical exacerbation. Recurrence of mucoid impaction in these segments is not rare and may predispose the patient to bronchial damage. High-attenuation mucoid impaction should be suggestive of ABPA [17, 78, 79] and recent data showed that it was associated with a more intense immunological activity [75].
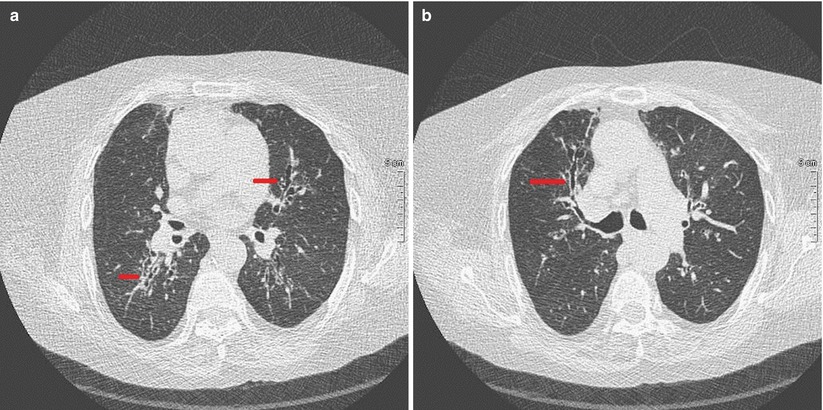
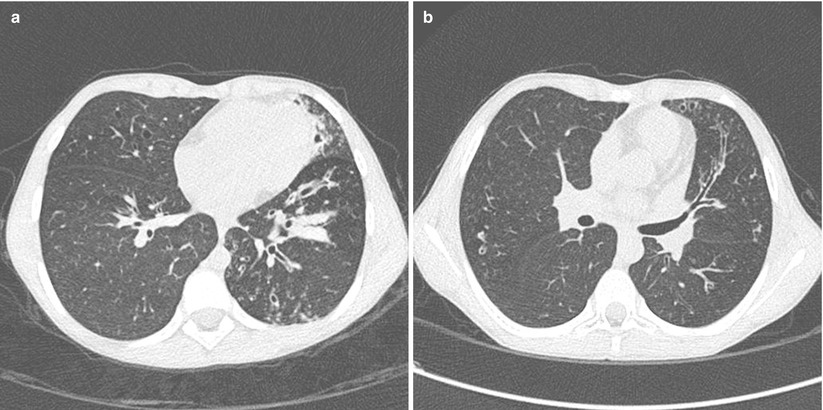
Fig. 5.3
(a, b) CT scan (lung window, 1 mm slices): proximal bronchiectasis (red lines) in a 62-year-old woman treated for bronchiectasis ABPA for 13 years
Fig. 5.4
(a, b) HRCT scan in a 13 years old girl with CF and ABPA: (a) tubular opacities and mucoid impaction (lower left lobe); (b) Bronchiectasis extending to the periphery with “finger in glove” appearance (lingula)
Pleural effusion or calcifications of mucoid impactions are rare but have been reported [80]. Pulmonary fibrosis, pneumothorax and cavities occur during end-stage ABPA [76, 77, 81].
High-resolution CT scan is more sensitive than chest X ray for the detection of transient pulmonary infiltrate or bronchiectasis. Bronchiectasis patterns are described as cylindrical in most cases, but have also been referred to as cystic or varicose [81, 82]; Several studies have compared abnormalities in ABPA patients with those in Aspergillus-sensitive asthmatics [8, 81–85]. One of those studies showed that bronchiectasis is common in ABPA but occurs only occasionally in asthmatic adults with a positive skin test to AF [83]. In that study, bronchiectasis was identified in 14/17 ABPA patients (82 %) with a large percentage of lobes (42 %) versus 2/11 (18 %) asthmatics sensitized to AF and a low percentage of lobes (5 %). In that study, pleural thickening in 14 (82 %) and atelectasis in 9 (64 %) were also described [83].
Respiratory function tests (expiratory flow rates, lung volumes and diffusion capacities) are useful for diagnosis and during follow-up, but alone are not sufficient for monitoring treatment. Obstruction and restriction are both aggravated during acute exacerbations. Reductions in lung volume and diffusion capacity have been observed during exacerbations and in patients with end-stage ABPA [4, 86]. The severity of the obstruction in corticosteroid-dependent asthma (stage IV) varies depending on the patient [87–89]. Deterioration of lung function also differs between ABPA patients; in some individuals, lung function remains stable, or is even improved in serologic ABPA (without bronchiectasis) [90], whereas in others, functional parameters progressively deteriorate [91]. In CF patients, ABPA is associated with a more severe progression of forced vital capacity (FVC) and forced expiratory volume in one second (FEV1) [92]. Malo et al. compared the results of lung function tests of 20 asthmatic patients with ABPA with those of 20 asthmatics, paired in terms of sex, age and duration of asthma [93]. All patients with ABPA and 75 % of patients with asthma alone showed significantly reduced FEV1. In contrast, FEV1 reversibility was more frequent in patients with asthma alone (50 %) than in those with ABPA (31 %), and the extent of this reversibility was also statistically higher in patients with asthma compared with those with ABPA [93].
Skin Tests and Biological Investigations
Nearly all ABPA patients show an immediate cutaneous reaction to skin prick-tests with an Aspergillus mixture (aspergillus allergens extracts). The reactivity varies in time and may be influenced by the allergenic extracts. A dual reaction (associated immediate and late or delayed positive skin tests) is rare, involving about 16–33 % of patients [94, 95]. The delayed reaction is of little interest in ABPA diagnosis [94, 95]. Concerning the use of recombinant antigens in cutaneous testing, Hemmann et al. showed that skin prick tests with rAspf4 and rAspf6 provoked immediate skin reactions in patients with ABPA but not in controls, and therefore enabled discrimination between ABPA and sensitisation to A fumigatus [96].
Patients may also have sputum and/or blood eosinophilia, particularly at the time of diagnosis or when exacerbations occur during periods when they are not receiving corticosteroids. In these situations, blood eosinophil levels may be high, between 1,500 and 3,000/mm3 [95].
A fumigatus can be detected in the sputum of 50 % of ABPA patients [95]. Examinations of two or more specimens increase the rates of positive culture [97]. Aspergillus PCR, more sensitive than culture, may be efficient in evaluating the effectiveness of antifungal therapy, but has poor interest in ABPA diagnosis [98]. The presence of hyphae is more specific than spores.
The most reliable diagnostic tests are measurements of total serum IgE and serum IgE- and IgG- specific antibodies as well as the determination of the presence of A. fumigatus antibody precipitins (results expressed as the number of precipitation lines). It generally shows two or more precipitation lines, to one or sometimes more extracts [99]. Extracts differ between laboratories. Some Aspergillus antigens (catalase, trypsine, chymotrypsine) are essential for these reactions. These enzyme activities can be detected after gel diffusion and, as these antigens appear to be specific to A. fumigatus, may be useful for diagnosis [100]. Variations in levels of specific antibodies are a function of treatment, age and stage of ABPA [101–103]. Total serum IgE levels are high in ABPA patients, usually greater than 1,000 IU/mL and decrease when they are in remission as a result of corticosteroid treatment. This decrease occurs within 2 months after initiation of corticosteroid treatment. Total serum IgE levels sometime return to within the normal range during the end-stage [101].
Approximately 60 epitopes able to bind the IgE molecules have been identified from A. fumigatus, alongside more than 20 recombinant allergens (named Aspf1 to Aspf22) [99]. Studies suggest that some of the recombinant allergens may be useful for discriminating between individuals with ABPA and those with AF-sensitised asthma [45]. Kurup et al. assessed the abilities of recombinant Aspergillus allergens (Aspf1, f2, f3, f4, and f6) from the sera of ABPA patients and A. fumigatus-sensitive asthmatics to bind to IgE: the number of recombinant allergens able to bind to the IgE antibody was higher in sera from patients with ABPA than in those of the asthmatics. Aspf2, f4, and f6 interacted with IgE in all ABPA patients tested [45]. Such binding tests could therefore be used in ABPA diagnosis. In contrast, IgE antibodies binding to Aspf1 and f3 were not specific. Several studies compared the respective responses in terms of specific IgE antibodies towards the recombinant A. fumigatus antigens (mainly Aspf2, f3, f4, f6 and f16) in asthmatics sensitised to A. fumigatus and in ABPA patients with or without CF. Current results show some discrepancies. Crameri et al. reported higher IgE levels to rAspf4 and f6 in ABPA patients when compared with asthmatics sensitised to Aspergillus [104]. The same group showed that specific IgE to rAspf1 and f3 represented a marker for sensitisation, while specific IgE antibodies rAspf4 and f6 gave an indication for ABPA which was clinically confirmed [105].
Hemmann et al. also reported higher IgE levels to Asp f4 and f6 in ABPA CF patients [105]. Another study analysed the position of different recombinant antigens in their binding to IgA, IgG and IgE antibodies in patients with CF alone or associated with ABPA [106]. Present data suggest that no antigen (rAspf1, 2, 3, 4, 6), antibody isotype or method is capable of differentiating CF with or without ABPA, although some allergens show a higher prevalence of strong reactions. Recombinant allergens, rAspf1, rAspf2, rAspf3, rAspf4 and rAspf6 and recently rAspf34 have been evaluated to differentiate ABPA from asthma-sensitised to AF and mainly to diagnose ABPA in CF [63, 106–108]. Banerjee et al. showed that 70 % of patients with ABPA had high levels of serum IgE antibodies to Aspf16, a 43 kDa protein, whereas patients with positive AF skin test did not [109]. Specific serum IgE from rAspf4 and rAspf6 seems to be detected only in ABPA, but other studies did not show this [110]. The sensitivities obtained seem to be higher with rAspf4 [107, 111]. Only Latzin [63] showed a higher sensitivity with rAspf6 compared with rAspf4; rAspf6 is specifically expressed in hyphae, which might explain a preferential IgE response to rAspf6 in ABPA patients [112].
Two additional points must be discussed in patients with ABPA: amplification of the total IgE response appears to be associated with the presence of abundant amounts of carbohydrates present in the mould Aspergillus, but carbohydrates only act as an adjuvant and are not the target of the induced IgE response [67]. Similarly, the kinetics of the antibody response to recombinant antigens in ABPA patients showed serum levels of specific IgE 16–18 times higher than rAspf4 and f6, but follow-up of the specific IgE response was of limited value for guiding therapy [113]. To conclude, even if rAspf2 and rAspf4 and rAspf6 are more often associated with ABPA, their lack of specificity do not yet permit to use them in clinical routine, in asthma as in CF If recombinant allergens are available, their usefulness in the diagnosis work up needs to be confirmed.
Other markers such as TARC, elevated in CF patients with ABPA, are not routinely evaluated.
Pathology of ABPA
Although pathological specimens are obviously not necessary for diagnosis, when bronchial samples were studied, the bronchial tree was dilated and filled with mucus plugs containing macrophages, eosinophils, Charcot-Leyden crystals and sometimes hyphae or hyphal fragment [114, 115]. Bronchial walls were infiltrated with inflammatory cells (eosinophils, lymphocytes and plasma cells); a thickening of the basement membrane along with epithelial abrasion was also found. The pathology of the peribronchial areas and parenchyma is sometimes different from that described above: bronchocentric granulomatosis with bronchial remodelling and dilation has been described as being a complication of ABPA [116]. However, bronchocentric granulomatosis is clearly a particular entity associated with a different pseudo-tumoral radiological pattern and possibly with other conditions such as tuberculosis, inflammatory disease of the bowel and rheumatoid arthritis [117]. Infiltration of the parenchyma with mononuclear cells, eosinophils and lymphocytes leads to inflammation that mimics or is associated with patterns observed in individuals with other forms of interstitial disease such as granulomatous bronchiolitis, exsudative bronchiolitis or obliterans bronchiolitis [118]. Micro-abscesses with Aspergillus hyphae and granulocytes have also been described in the parenchyma of ABPA patients, demonstrating that the frontier between invasive and allergic manifestations is sometimes poorly delimited.
Diagnostic Criteria and Stages in Asthmatics and in CF Patients
The diagnosis of ABPA is based on the presence of a combination of clinical, biological and radiological criteria.
When the patient is under corticosteroids, some parameters can be modified: disappearance of pulmonary infiltrate, of blood eosinophilia, and decrease of total IgE and antigens directed to AF. For these reasons, it is sometimes useful to re-test the patient at distance from systemic corticosteroids.
In asthma, bronchiectasis involving the more central segmental bronchi is a strong diagnostic criterion, but is not always present in patients during follow-up or at the time of diagnosis. Greenberger identified two groups for differentiating ABPA patients, with and without bronchiectasis [119]: ABPA with central bronchiectasis and seropositive ABPA without bronchiectasis. The “major” and “minor” criteria are challenged, because the value of these criteria is not established (positive and negative predictive values). For this reason, minimal criteria to diagnose ABPA should be retained (Table 5.2). Kumar et al. [120] studied the characteristics of ABPA patients and found that patients could be divided into three groups: ABPA with positive serology (ABPA-S), ABPA with central bronchiectasis (ABPA-CB) and ABPA with central bronchiectasis and other radiologic features (ABPA-CB-ORF). Pulmonary function abnormalities were mild in the ABPA-S group, moderate in the ABPA-CB group and severe in the ABPA-CB-ORF group. Absolute eosinophil counts rose in each group, but were highest (1.233/ml) for the ABPA-CB-ORF group. The levels of A. fumigatus-specific IgE followed the same pattern, with a maximum of 47.91 KIU/L for the ABPA-CB-ORF group. Symptom scores were also higher for the ABPA-CB-ORF group than for the other groups. Thus, the ABPA-S group probably comprised patients at an early stage or with a less aggressive form of ABPA. Studies by Greenberger et al. [99, 119] led them to suggest that early recognition and treatment of ABPA may prevent progression to end-stage ABPA. A recent study [17] evaluated 564 patients with asthma screened for Aspergillus with skin tests. 223 (39.5 %) had positive AF skin tests. ABPA was diagnosed in 126 patients (27 %). Among this population, there was 27 % ABPA-S, 33 % ABPA-CB and 40 % ABPA-CB-ORF with radiological findings. An interesting point is that there was no difference between the stage of ABPA and the severity of asthma, the duration of illness or serologic findings. However, tuberculosis was diagnosed in the past in 46.8 % of this population [17]. For this reason, these data cannot be superimposed on countries with low-endemic tuberculosis.
In CF patients: ABPA is a common complication of this disease, occurring in approximately 10 % of cases. Diagnosis of ABPA in CF patients is difficult for several reasons. Some of the criteria used for ABPA diagnosis are common manifestations of CF. CF patients often present exacerbations with bronchial obstruction, pulmonary infiltrate and bronchiectasis [9, 121]. In addition, CF patients may develop immune responses to Aspergillus (IgE, IgA, IgG antibody production, elevated total serum IgE levels) in the absence of ABPA. The boundary separating these biological responses from those involved with ABPA is extremely difficult to define [122–124]. Recently, the CF Foundation has proposed a new set of criteria for ABPA diagnosis in CF patients [9] (Table 5.3). These criteria are particularly valuable for diagnosis in cases where the condition of the patient has only slightly improved, or not improved at all, after appropriate treatment for bacterial bronchial infection. It is recommended that CF patients be screened for ABPA (serum total IgE, specific IgE/AF and precipitins/AF) from the age of 6, once a year or in response to the clinical suggestion of ABPA [9]. The prevalence of ABPA was low in patients under 6 years of age. In the European epidemiological study reported by Mastella et al., ABPA was more common in patients with a poorer clinical condition (lower FEV1, higher rate of microbial colonisation, poor nutritional status) [12]. Most of these patients had a delta f508/delta f508 genotype [12]. Due to this strong association between CF and ABPA, it may be useful to perform sweet chloride tests on patients showing signs of ABPA. In some patients, CF was diagnosed at the same time as ABPA [125].
ABPA progresses in five stages, which are not consecutive in time [13, 99] listed in Table 5.4. Treatment differs depending on the ABPA stage. Patients with acute exacerbation respond to corticosteroids and early treatment of pulmonary infiltrate with these drugs may prevent bronchial or bronchiolar destruction. Long-term treatment with corticosteroids is not recommended because this treatment does not prevent the emergence of new infiltrates or progression to fibrosis. Measuring total serum IgE levels is helpful for monitoring the treatment regimen. Total serum IgE levels are high during the acute and exacerbation phases of ABPA. By the end-stage, prognosis and treatment resemble those for CF patient management: patients have extensive bronchial destruction and the bronchial tree may be colonised by Staphylococcus aureus and/or Pseudomonas aeruginosa. Response to corticosteroids is limited at this stage. However, progression from stage I to stage V is not unavoidable and progression from stage IV to V is particularly uncommon.
Table 5.4
Stages of ABPA
Stage | Clinical characteristics | Biology | Radiology |
|---|---|---|---|
I: Acute | Fever, cough, chest pain, hemoptysis, sputum | Elevated total serum IgE +++ levels, (+/−blood eosinophilia) | Pulmonary infiltrate (s) (upper/middle lobes) |
II: Remission | Asymptomatic/stable asthma | Normal or elevated total serum IgE + levels | No infiltrates, in the absence of systemic corticosteroid therapy for >6 months |
III: Exacerbation | Symptoms mimicking the acute stage or asymptomatic | Elevated total serum IgE +++levels, (+/−blood eosinophilia) | Pulmonary infiltrate(s) (upper/middle lobes) |
IV: Cortico-dependent asthma | Persistent severe asthma | Normal or elevated total serum IgE + levels | With or without pulmonary infiltrate(s) |
V: Fibrosis (end-stage) | Cyanosis, severe dyspnea | Normal or elevated total serum IgE + levels | Cavitary lesions, extensive bronchiectasis, fibrosis |
Differential Diagnosis or Overlap Syndrome?
Asthma with Fungal Sensitisation
The main difficulty is differentiating between asthma with fungal sensitisation and ABPA. About 20–25 % of patients with persistent asthma are sensitised to one or more fungi [30, 126–128]. Among 1,132 asthmatics, sensitisation to Alternaria or Cladosporium increased the risk of severe asthma [129]. Adults with asthma having been admitted to hospital for acute asthma at least twice were more likely to be skin-test positive for at least one of the moulds AF, Penicillium notatum, Cladosporium herbarum, Alternaria alternata or Candida albicans (76 %) compared with mild to moderate asthma-sufferers (16–19 %; p, 0.0001) [130]. Another study also showed a doubling of the frequency of mould-positive radioallergosorbent tests (RASTs) in the moderate and severe groups (FEV1: 31–35 % of predicted value) compared with mild and no asthma controls (17–19 %; p = 0.01). A. fumigatus detection in sputum of asthmatics is associated with A. fumigatus-IgE sensitisation, neutrophilic airway inflammation and reduced lung function (FEV1 and FVC) [131]. The borderline between asthma and seropositive ABPA is sometimes difficult to identify when more than 10 % of asthmatic patients have precipitins directed/AF [132]. At least, one study showed that anti-fungal therapy may improve asthma in patients sensitised to AF [133]. This study and the high rate of AF sensitization in severe asthma explain that the term “severe asthma associated with fungal sensitization” (SAFS) is now discussed [133].
Allergic Aspergillus Sinusitis
The symptomatic search for sinus localisation is recommended. In a series of 95 patients with ABPA, Shah et al. [134], showed radiological evidence of sinusitis in 22 cases and confirmed, by antral wash or a surgical approach, the presence of Aspergillus in 7 cases. The same group [135] recently reported the coexistence of ABPA, allergic Aspergillus sinusitis and aspergilloma in the same patient, an association that we also observed in two patients some years ago (personal unpublished data). Bone erosions are described on CT scan and specific ear-nose-throat (ENT) evaluation is required.
Hypersensitivity Pneumonitis (HP)
HP is an interstitial lung disease, that may result of an immune reaction (type III and IV hypersensitivity) to inhaled fungi (Penicillium fusarium, Trichosporon… and also Aspergillus species, such as AF, A clavatus, A versicolor). Most HP related to fungi occur in an occupational setting. HP related to A clavatus and A fumigatus are well described in the “malt-worker’s lung” and AF is implicated in farmer’s lung, salami brusher’s lung, and in HP in tobacco industries [136–138]. Except for the summer-type HP causes by Trichosporon species in Japan, HP related to domestic fungi exposure is rare [139, 140]. Chronic HP caused by AF because of domestic leaky walls, resulting in lung fibrosis has been recently reported in Japan [141]. Implication of fungi have also been discussed in “humidifier lung”, but the role of endotoxins and bacteria are also mentioned [142]. Insidious or acute presentations are reported, depending on the intensity and duration of exposure. Clinical symptoms (malaise, sweating, myalgia, loss of weight, and/or dyspnea), associated with micronodular and/or ground-glass opacities on CT scan in a particular environment and the identification of serum precipitins to AF extracts (usually present), or other fungi lead to diagnosis [143]. Serum precipitins to mould antigens have a controversial value for HP diagnosis. Fenoglio et al. suggest, with the aim to improve their diagnostic value, to use serological scores with a panel of relevant antigens [144]. Removal of the patient from exposure, and corticosteroids for severe patients usually lead to prompt resolution.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


