Evidence for the use of airway clearance techniques is often difficult to evaluate, in part due to agreement that top-level evidence on this topic is lacking.1a–b The components of a given treatment have not been standardized and the literature refers to ACTs using a variety of terms, including chest physiotherapy, chest physical therapy (CPT), bronchial drainage, postural drainage (PD) therapy, and bronchial hygiene. In addition, the availability of equipment and cultural differences in its application confound research results. Differences in the outcome measures for a given technique also occur—some studies use wet or dry (dehydrated) sputum volume or radioaerosol clearance, whereas other studies use pulmonary function tests, radiographic evidence, or arterial blood gases to asses the effectiveness of a specific technique. The majority of secretion clearance research has been focused on patients with cystic fibrosis, as the need for ongoing secretion removal is apparent in this population. However, results showing a treatment to be effective in one cross section of patients must not be generalized to apply to the treatment across all patients with pulmonary disease. Historically, the gold standard of airway clearance has been a combination of postural drainage, percussion, and vibration with cough. This has been challenged1b–c as more techniques have been demonstrated to be effective. Postural drainage and percussion have been shown to be ineffective in some cases and, in fact, to be detrimental to pulmonary status in others. Caregivers have also been shown to suffer from the performance of percussion; repetitive-motion injuries of the wrists have been documented as a result of regular performance of percussion.2,3 Alternative techniques have arisen out of the need to find effective methods for those patients not responsive to traditional methods. A desire to increase adherence with airway clearance, especially in patients approaching adolescence and adulthood, has led to an investigation of more independent techniques.4 Many of these techniques have been practiced longer in other countries, but are now commonly used by practitioners in the United States. It is important to remember, however, that secretion clearance is just one step toward realizing effective gas exchange in the complex oxygen transport pathway.5 Airway clearance, when indicated, should be integrated into a comprehensive plan of care, including positioning and mobilization, to optimize oxygen transport. Oxygen transport is the primary purpose of the cardiopulmonary system (see Chapter 2). Ventilation of the alveoli is an important step in the oxygen transport chain; it allows optimal delivery of oxygen to the tissues. Several medical and surgical conditions may interfere with this process. Retained secretions or mucus plugs in the airways may interfere with the exchange of oxygen. The secretions must be mobilized from the peripheral, or smaller, airways to the larger, more central airways, where coughing or suction may remove them. In this multisystem genetic disease of exocrine gland dysfunction, copious (often purulent), thick secretions and mucus plugs block the peripheral and central airways. Even infants diagnosed with cystic fibrosis, whether symptomatic or not, show evidence of small airway obstruction in the form of bronchial mucus casts.6 Recurrent bacterial infections combined with this mucus hypersecretion in the lungs leads to destruction of the bronchial walls, or bronchiectasis. Airway clearance is recommended for all patients with CF and continues to be an important therapy in the treatment of cystic fibrosis.1b,6a This practice is supported by evidence of deteriorating lung function when regular treatments of postural drainage and percussion have been stopped.7,8 This condition results in a breakdown of the elastic tissue in the bronchial walls, causing severe dilation. Inflamed mucosa and copious purulent secretions are present in this condition. Airway clearance has been shown to benefit patients with bronchiectasis in the mobilization of sputum.9,10 This condition is caused by the collapse of alveolar segments, often by retained pulmonary secretions. It has been documented in patients who have undergone surgery under general anesthesia, especially in cases of thoracic or abdominal surgery. ACTs are indicated in cases of atelectasis due to mucus plugging.11,12 Many patients with neurological or metastatic diseases or general debilitation tend to hypoventilate or have increased work of breathing. They are unable to maintain adequate control of respiratory secretions and often have weak, ineffective coughing mechanisms.13 This is especially true in patients with diminished diaphragm innervation resulting from spinal cord injuries.14 Patients requiring ventilatory support for any reason, including patients who are obtunded or comatose, are at risk for atelectasis and are unable to manage their secretions independently.15 Airway clearance is considered standard practice in the management of patients on mechanical ventilation.15a These infants are born lacking surfactant in the lungs, which results in atelectasis. ACTs may be useful in clearing secretions and preventing atelectasis, but there should be a clear indication for this procedure and it must be monitored carefully in this population.16,17 This condition is characterized by the presence of hyperreactive airways and mucus plugging. ACTs may be beneficial to assist in the mobilization of mucus plugs but are not helpful in treating uncomplicated acute exacerbations.18 There are several conditions that do not appear to benefit from ACTs. Patients with pneumonia or chronic bronchitis without large amounts of secretion production do not appear to benefit from airway clearance. No differences in outcome were found when these populations were treated with postural drainage and percussion.19–22 Viral bronchiolitis is an asthma-like lung disease occurring in infants less than 2 years of age. These patients do not appear to benefit from ACTs.23 Also of little benefit, and possibly harmful, is the inclusion of airway clearance in the routine care of postoperative patients without extensive secretions.18 Even in patients with a history of lung disease, the use of ACTs has failed to affect the incidence of atelectasis as a postoperative complication.24 In addition to improving many outcomes in patients with lung disease, exercise has been shown to assist in secretion clearance.25–28 Exercise increases mucociliary transport in patients with chronic bronchitis.28 Higher transpulmonary pressure with aerobic exercise may open closed bronchi, as well as increase collateral ventilation to allow mucus to be moved.26 It has also been shown that exercise-induced hyperventilation is more effective than eucapnic hyperventilation in mobilizing bronchial secretions.29 The contribution of increased expiratory airflow and exercise-induced coughing are other factors in improving secretion removal. Exercise for secretion clearance has focused on aerobic or endurance exercise; however, any form of exercise must be adapted to the individual patient’s status and abilities. Based on a lack of decrease in lung function following the cessation of PD and percussion but the continuation of an exercise program, or based on the improvement in pulmonary function, exercise has been recommended as a replacement for a conventional chest physiotherapy routine in some patients or at some stages of lung disease.26,27,30,31 In hospitalized patients with cystic fibrosis, no significant change in pulmonary function was reported when exercise was substituted for two of three daily treatments of PD, percussion, and vibration, and the weight of the sputum produced was equivalent.30 In terms of mucus cleared, no significant differences were found among exercise on a cycle ergometer, postural drainage, and PEP mask breathing.32 Increases in sputum expectoration on exercise days as opposed to nonexercise days have also been reported.27,33 However, other studies conclude that exercise alone is not sufficient and recommend its use as a complement to other forms of airway clearance. Airway clearance using PD and FET was shown to be more effective than exercise with a cycle ergometer in inducing sputum expectoration.34 Results from Bilton and colleagues35 demonstrated that any modality that included the active cycle of breathing technique (ACBT) in PD positions alone or in combination with exercise is better than exercise alone at clearing sputum. It is difficult to compare these studies, however, because the mode and length of exercise differ, as do the outcome measures of effectiveness of airway clearance. Exercise as an airway clearance technique is not suitable for the very young (younger than 4 to 5 years of age), for patients with neuromuscular limitations, or for patients with limited exercise tolerance. Moreover, the potential need for supplemental oxygen during exercise should be monitored. Nonetheless, evidence suggests that an exercise program, in addition to clearing secretions, may decrease morbidity and mortality by improving exercise capacity.36,37 Exercise has the advantage of being the only airway clearance technique that is performed regularly by people without lung disease. This factor can make it appealing to those patients who do not want to call attention to their differences from their peers. Exercise may improve self-esteem, a sense of well-being, and quality of life. Higher levels of exercise tolerance in patients with cystic fibrosis have been demonstrated to improve survival.37 Some patients may not tolerate the amount or frequency of exercise necessary for this to be the sole method of airway clearance. Thus various airway clearance techniques can be used as adjuncts to exercise. This is particularly true during an acute exacerbation when activity tolerance is limited, or in infants or patients with neurological or musculoskeletal limitations. Andreasson26 observed that regular contact with a caregiver seems to be necessary for successful exercise training, as does family support, especially in young children. This points out the difficulty with adherence to a home program. Adherence will also be affected by a patient’s preference for a particular activity, scheduling conflicts, and commitment by friends and family members. Several precautions must be observed when using exercise as a form of airway clearance. Care must be taken in prescribing exercise to patients with hyperreactive airways or a tendency toward oxygen desaturation. Desaturation has been shown to occur with exercise in individuals with pulmonary disease,38,39 and therefore it becomes prudent to monitor oxygen saturation, providing supplemental oxygen for the exercise period when indicated. Exercise-induced bronchospasm must also be considered when pulmonary compromise is seen with exercise, especially with higher-intensity exercise.40 When medication is indicated, it is recommended to provide an inhaled bronchodilator 20 to 30 minutes before exercise to alleviate this symptom.41 Use of bronchodilator medication and supplemental oxygen may be necessary to improve exercise tolerance, but these patients require closer monitoring as well. Andreasson26 reports a risk for pneumothorax associated with exercise in patients with extensive bullae. In patients who are very young, who have limited ability to cooperate, or who are not adherent to other ACTs, percussion, shaking, and vibration offer methods for dislodging retained secretions. However, because of the force transmitted to the thoracic cage with these techniques, there are many precautions and contraindications to consider. The therapist should not make this decision alone but should seek direction from the medical team. These treatments are not completely benign and should not be performed in the absence of good indications.42 Percussion has been shown to contribute to a fall in PaO2 in acutely ill patients,43 especially in patients with cardiovascular instability44 and in neonates.45 The factor that seems most closely associated with or predictive of this effect is the patient’s baseline PaO2.42 Cardiac dysrhythmias have been associated with chest percussion for bronchial drainage11 and Huseby46 hypothesizes that hypoxemia may be the underlying mechanism of CPT-caused cardiac arrhythmias. Patients with hyperreactive airways (e.g., asthma) show intolerance for percussion as part of airway clearance. Campbell and colleagues47 demonstrated a fall in FEV1 associated with percussion; it was not evident when percussion was omitted. Administration of a bronchodilator before treatment with percussion precluded the fall in FEV1. Wheezing has also been associated with percussion and vibration in patients with cystic fibrosis and COPD.48,49 Box 21-1 summarizes the precautions and contraindications for external manipulation of the thorax associated with percussion, shaking, and high-frequency chest compression. Vibration involves less force to the thorax and may be better tolerated than the aforementioned techniques. A nebulized bronchodilator may be administered during a treatment of high-frequency chest compression to avoid the consequences of hyperreactive airways. Box 21-1 Contraindications to External Manipulation of the Thorax in Addition to Contraindications for Postural Drainage From AARC Clinical Practice Guideline: Postural drainage therapy, Respiratory Care 36:1418-1426, 1991; and Crane L: Physical therapy for the neonate with respiratory disease. In Irwin S, Tecklin JS, editors: Cardiopulmonary physical therapy, St. Louis, 1985, Mosby. Postural drainage, also known as bronchial drainage, is a passive technique in which the patient is placed in positions that allow gravity to assist with the drainage of secretions from the bronchopulmonary tree. PD is accomplished by positioning the patient so that the angle of the lung segment to be drained allows gravity to have its greatest effect (Figure 21-2). Positioning the patient to assist the flow of bronchial secretions from the airways has been a standard treatment for some time in patients with retained secretions.50 Knowledge of the anatomy of the tracheobronchial tree is vital to effective treatment. Each lobe to be drained must be aligned so that gravity can mobilize the secretions from the periphery to the larger, more central airways. The mechanism of postural drainage is considered to be a direct effect of gravity on bronchial secretions, although observations made by Lannefors (1992)32 that gravity also influences regional lung ventilation and volume suggest that these mechanisms are also involved. PD has been shown to be effective in mobilizing secretions in patients with cystic fibrosis,51,52 bronchiectasis,10 and other pulmonary diseases.53,54 Other treatments, such as percussion, vibration, and the active cycle of breathing technique (ACBT), may be used while the patient is in postural drainage positions. It is essential that the therapist and the health care team discuss treatment priorities when deciding to use PD positions. A decision to use postural drainage might be made despite a contraindication if the benefits are thought to outweigh the risks in a particular case. For example, it is known that use of the Trendelenburg (head-down) position increases intracranial pressure in patients after neurosurgery.56 However, if the patient develops atelectasis, the stress of respiratory embarrassment may also increase intracranial pressure. In this instance, the decision may be made to position the patient to clear the atelectasis and subsequently return to a modified conservative regimen.55 A fall in arterial O2 saturation has been reported with the use of postural drainage for airway clearance, although the effects of PD were not separated from additional techniques.46,57 Therefore O2 saturation levels should be monitored during treatment, especially in patients with known low PaO2 values. Caution must also be used in treating a patient with end-stage lung disease in postural drainage positions because of the risk for hemoptysis.58,59 Decreased cardiac output60,61 has been associated with chest physiotherapy treatment; however, the effects of postural drainage were not separated from those of percussion and vibration. Many physical therapists working with the pediatric population almost never use the head-down position in treating infants but rather a modified routine that excludes the Trendelenburg position. The head-down position has been shown to increase the incidence of gastroesophageal reflux in neonates.16 Button and colleagues62 found that the head-down position is associated with gastroesophageal reflux, distressed behavior, and lower oxygen saturation in infants with cystic fibrosis. It should be noted that a finding of gastroesophageal reflux can occur even 1 hour after treatment. A modified routine that eliminates head-down positioning is associated with fewer respiratory complications.63 Box 21-2 summarizes the precautions and contraindications concerning postural drainage. Box 21-2 Contraindications for Postural Drainage All Positions Are Contraindicated for the Following From AARC Clinical Practice Guideline: Postural drainage therapy, Respiratory Care 36:1418-1426, 1991; and Crane L: Physical therapy for the neonate with respiratory disease. In Irwin S, Tecklin JS, editors: Cardiopulmonary physical therapy, St. Louis, 1985, Mosby. Percussion, sometimes referred to as chest clapping, is a traditional approach to secretion mobilization. A rhythmical force is applied with a caregiver’s cupped hands against the thorax, over the involved lung segments, trapping air between the patient’s thorax and the caregiver’s hands (Figure 21-3), with the aim of dislodging or loosening bronchial secretions from the airways so they may be removed by suctioning or expectoration. This technique is performed during both the inspiratory and expiratory phases of breathing. Percussion is used in postural drainage positions for increased effectiveness64,65 and may also be used during ACBT. For individuals with pulmonary disease, percussion in conjunction with postural drainage continues to be a mainstay of the treatment, especially for pediatric patients and patients who are unresponsive. The proposed mechanism of action of percussion is the transmission of a wave of energy through the chest wall into the lung. This wave loosens secretions from the bronchial wall and moves them proximally, where ciliary motion and cough (or suction) can remove them. The combination of postural drainage and percussion has been shown to be effective in secretion removal.66–68 A handheld mechanical percussor can be used by a caregiver to minimize fatigue or may be used by the patient to self-administer percussion. The effectiveness of mechanical as opposed to manual percussion has been studied. Maxwell and Redmond69 found mechanical percussion equivalent to manual percussion in effecting removal of secretions. Although there was a significant increase in pulmonary function with manual techniques, Pryor and colleagues70,71 supported the use of mechanical percussion in patients, using the forced expiration technique. A study by Rossman and colleagues72 was in disagreement, finding that mechanical percussion did not enhance postural drainage in secretion removal. Percussion is not well tolerated by many patients postoperatively without adequate pain control. The force of percussion may also be contraindicated in patients with osteoporosis or coagulopathy. Percussion has been associated with a fall in oxygen saturation, which can be eliminated with concurrent thoracic expansion exercises and pauses for breathing control.75 It is proposed that vibration and shaking enhance mucociliary transport from the periphery of the lung fields to the larger, central airways. Because the compressive force to the thorax is greater with shaking than vibration, it produces increased chest wall displacement, and the stretch of the respiratory muscles may produce an increased inspiratory effort and lung volume.76 The same relative contraindications for percussion should be observed for shaking, because it involves the application of force to the thorax. Pavia77 demonstrated a higher, though not statistically significant, rate of secretion clearance and sputum production with vibration. However, this study was conducted while subjects were in the upright position only, which does not replicate the use of vibration clinically. Many studies do not separate the effects of vibration from the components of PD and percussion because they are often used in conjunction. In fact, many studies describe the techniques of PD, percussion, and vibration or shaking as a single entity and refer to the treatment as chest physical therapy or postural drainage therapy. Mackenzie and colleagues78 demonstrated significant improvement in total lung/thorax compliance after treatment with postural drainage, percussion, and vibration in mechanically ventilated patients. Feldman and colleagues48 demonstrated improved ventilatory function by improved expiratory flow rates in patients receiving postural drainage, percussion, vibration, and directed coughing. The technique of manual hyperinflation was used more commonly in the past for patients requiring mechanical ventilation. However there is not enough evidence to promote the regular use of this technique that has many contraindications and that is not well known in the United States.80 A brief description of the technique and its precautions follows. Two caregivers are needed to perform the technique with the patient placed in PD positions.79 One caregiver uses a manual inflation bag to hyperinflate the lungs with a slow, deep inspiration and, after a short pause, provides a quick release to allow rapid exhalation. A second caregiver applies shaking or vibration at the beginning of exhalation to mobilize secretions. The technique is promoted to mobilize secretions and reinflate collapsed areas of the lung and is likened to simulating a cough—deep inspiration, pause, and forceful exhalation. Clement80 reported that this method of airway clearance enabled patients to be maintained on ventilators for long periods while retaining normal lung function. It was also demonstrated that the addition of positioning and vibrations enhanced the treatment of atelectasis by hyperinflation and suctioning.81 The risks to using manual hyperinflation are numerous. There are several adverse hemodynamic effects of this technique and hyperinflation has the potential to cause barotraumas.61,80,83
Airway Clearance Techniques
Conditions That May Indicate Airway Clearance
Cystic Fibrosis
Bronchiectasis
Atelectasis
Respiratory Muscle Weakness
Mechanical Ventilation
Neonatal Respiratory Distress Syndrome
Asthma
Airway Clearance Techniques
Exercise for Airway Clearance
Treatment with Exercise
 A walking program requires only a suitable pair of shoes and a safe location. Higher-impact exercise, because of increased stress on the knees, requires shoes specifically for that purpose. Clothing should be appropriate for the weather if exercising outdoors.
A walking program requires only a suitable pair of shoes and a safe location. Higher-impact exercise, because of increased stress on the knees, requires shoes specifically for that purpose. Clothing should be appropriate for the weather if exercising outdoors.
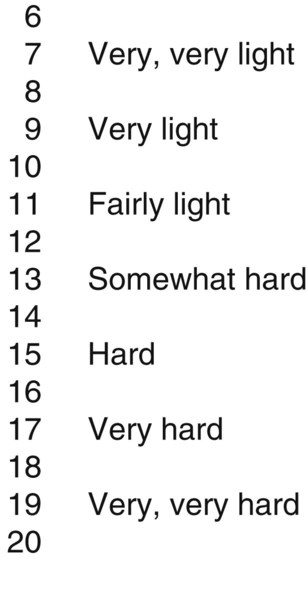
 Tools to monitor a patient’s response to exercise include a sphygmomanometer, stethoscope, heart rate monitor, pulse oximeter, and a scale to measure patient’s level of perceived exertion (Figure 21-1). In a home setting, patients should be knowledgeable in self-monitoring exercise intensity. For those patients who require closer monitoring, a pulse oximeter may be rented from an oxygen supply company. Monitoring of vital signs before and during exercise, and during recovery, will allow titration of the workload for optimal performance.
Tools to monitor a patient’s response to exercise include a sphygmomanometer, stethoscope, heart rate monitor, pulse oximeter, and a scale to measure patient’s level of perceived exertion (Figure 21-1). In a home setting, patients should be knowledgeable in self-monitoring exercise intensity. For those patients who require closer monitoring, a pulse oximeter may be rented from an oxygen supply company. Monitoring of vital signs before and during exercise, and during recovery, will allow titration of the workload for optimal performance.
Advantages and Disadvantages of Exercise
Precautions for Using Exercise
Contraindications and Precautions for Manual and Mechanical Airway Clearance Techniques
 Recent epidural spinal infusion or spinal anesthesia
Recent epidural spinal infusion or spinal anesthesia
 Recent skin grafts or flaps on the thorax
Recent skin grafts or flaps on the thorax
 Burns, open wounds, and skin infections of the thorax
Burns, open wounds, and skin infections of the thorax
 Suspected pulmonary tuberculosis
Suspected pulmonary tuberculosis
 Additional contraindications for percussion of a neonate
Additional contraindications for percussion of a neonate
Postural Drainage
Preparation for Postural Drainage
 For the hospitalized patient, electric beds allow patients to be positioned more easily. Air therapy beds, most often used in the intensive care unit (ICU), are valuable aids for positioning, especially in patients who are large or unresponsive.
For the hospitalized patient, electric beds allow patients to be positioned more easily. Air therapy beds, most often used in the intensive care unit (ICU), are valuable aids for positioning, especially in patients who are large or unresponsive.
 In the ICU, it is imperative to be familiar with the multiple lines, tubes, and other devices attached to the patient (see Chapter 16). Allow enough slack from each device to position a patient for postural drainage.
In the ICU, it is imperative to be familiar with the multiple lines, tubes, and other devices attached to the patient (see Chapter 16). Allow enough slack from each device to position a patient for postural drainage.
 Ensure there are enough staff members to position the patient with as little stress to both patient and staff as possible.55
Ensure there are enough staff members to position the patient with as little stress to both patient and staff as possible.55
 For treatment in the clinic, have foam wedges or pillows available for positioning.
For treatment in the clinic, have foam wedges or pillows available for positioning.
 For home treatment, aids in positioning might include pillows, sofa cushions, or a bean-bag chair.
For home treatment, aids in positioning might include pillows, sofa cushions, or a bean-bag chair.
 Nebulized bronchodilators or mucolytics before PD may facilitate the mobilization of sputum.
Nebulized bronchodilators or mucolytics before PD may facilitate the mobilization of sputum.
 For the patient with an adequate cough to expectorate secretions, have tissues or a specimen cup available. Have suctioning equipment ready to remove secretions from an artificial airway or the patient’s oral or nasal cavity after the treatment. Refer to Chapter 43 for a discussion of suctioning.
For the patient with an adequate cough to expectorate secretions, have tissues or a specimen cup available. Have suctioning equipment ready to remove secretions from an artificial airway or the patient’s oral or nasal cavity after the treatment. Refer to Chapter 43 for a discussion of suctioning.
Treatment with Postural Drainage
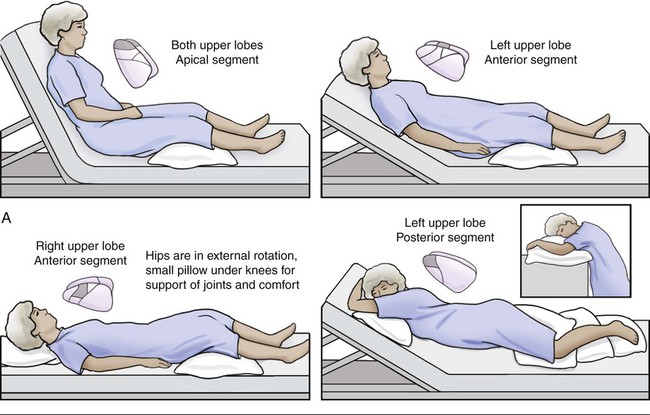
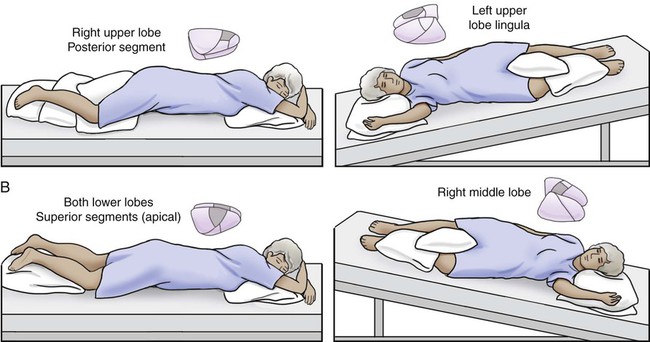
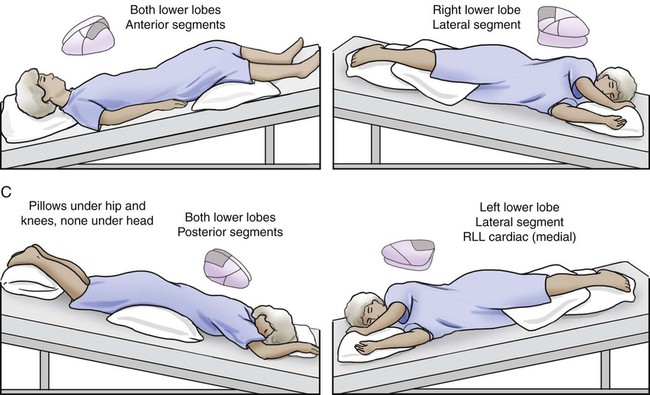
 After determining the lobe of the lung to be treated by auscultation and chest x-ray, position the patient in the appropriate position, supporting the patient comfortably in the position indicated (see Figure 21-2).
After determining the lobe of the lung to be treated by auscultation and chest x-ray, position the patient in the appropriate position, supporting the patient comfortably in the position indicated (see Figure 21-2).
 The patient should be encouraged to take deep breaths and cough after each position, if possible, and again after the treatment is completed. Having the patient sit upright or lean forward optimizes this effort by allowing the use of the abdominals for a stronger cough.55
The patient should be encouraged to take deep breaths and cough after each position, if possible, and again after the treatment is completed. Having the patient sit upright or lean forward optimizes this effort by allowing the use of the abdominals for a stronger cough.55
 Mobilization of secretions may not be apparent immediately after the treatment, but this may occur up to 1 hour later. The patient should be thus informed and reminded to clear secretions at a later time. A health care practitioner or family member should be included in this aspect of treatment, especially with patients who need encouragement.55
Mobilization of secretions may not be apparent immediately after the treatment, but this may occur up to 1 hour later. The patient should be thus informed and reminded to clear secretions at a later time. A health care practitioner or family member should be included in this aspect of treatment, especially with patients who need encouragement.55
General Precautions and Contraindications to Postural Drainage Positioning
 Intracranial pressure (ICP) >20 mm Hg
Intracranial pressure (ICP) >20 mm Hg
 Head and neck injury until stabilized
Head and neck injury until stabilized
 Active hemorrhage with hemodynamic instability
Active hemorrhage with hemodynamic instability
 Recent spinal surgery (e.g., laminectomy) or acute spinal injury
Recent spinal surgery (e.g., laminectomy) or acute spinal injury
 Pulmonary edema associated with heart failure (HF)
Pulmonary edema associated with heart failure (HF)
 Older, confused, or anxious patients
Older, confused, or anxious patients
 Rib fracture, with or without flail chest
Rib fracture, with or without flail chest
Percussion

Treatment with Percussion
 Position the hand in the shape of a cup with the fingers and thumb adducted. It is important to maintain this cupped position with the hands throughout the treatment, while letting the wrists, arms, and shoulders stay relaxed.
Position the hand in the shape of a cup with the fingers and thumb adducted. It is important to maintain this cupped position with the hands throughout the treatment, while letting the wrists, arms, and shoulders stay relaxed.
 The sound of percussion should be hollow as opposed to a slapping sound. If erythema occurs with percussion, it is usually a result of slapping or not trapping enough air between the hand and the chest wall.73
The sound of percussion should be hollow as opposed to a slapping sound. If erythema occurs with percussion, it is usually a result of slapping or not trapping enough air between the hand and the chest wall.73
 The patient will better tolerate an even, steady rhythm. The rate of manual percussion delivered by caregivers can vary between 100 and 480 times per minute.73
The patient will better tolerate an even, steady rhythm. The rate of manual percussion delivered by caregivers can vary between 100 and 480 times per minute.73
 The force applied to the chest wall from each hand should be equal. If the nondominant hand is not able to keep up with the dominant hand, the rate should be slowed to match that of the slower hand. It might be helpful to start with the nondominant hand and let the dominant hand match the nondominant hand.55 The force does not have to be excessive to be effective; the amount of force should be adapted to the patient’s comfort.
The force applied to the chest wall from each hand should be equal. If the nondominant hand is not able to keep up with the dominant hand, the rate should be slowed to match that of the slower hand. It might be helpful to start with the nondominant hand and let the dominant hand match the nondominant hand.55 The force does not have to be excessive to be effective; the amount of force should be adapted to the patient’s comfort.
 If the size of an infant does not allow use of a full hand, percussion may be done manually with four fingers cupped, three fingers with the middle finger “tented,” or the thenar and hypothenar surfaces of the hand.74
If the size of an infant does not allow use of a full hand, percussion may be done manually with four fingers cupped, three fingers with the middle finger “tented,” or the thenar and hypothenar surfaces of the hand.74
Advantages and Disadvantages of Percussion
Vibration and Shaking
Treatment with Vibration and Shaking
 For vibration, the hands may be placed side by side or on top of each other, as shown in Figure 21-4. As with shaking, the patient is instructed to take in a deep breath while in a proper PD position. A gentle but steady co-contraction of the upper extremities is performed to vibrate the chest wall, beginning at the peak of inspiration and following the movement of chest deflation. The frequency of manual vibration is between 12 and 20 Hz.44,53
For vibration, the hands may be placed side by side or on top of each other, as shown in Figure 21-4. As with shaking, the patient is instructed to take in a deep breath while in a proper PD position. A gentle but steady co-contraction of the upper extremities is performed to vibrate the chest wall, beginning at the peak of inspiration and following the movement of chest deflation. The frequency of manual vibration is between 12 and 20 Hz.44,53
 For shaking, with the patient in the appropriate PD position, place your hands over the lobe of the lung to be treated and instruct the patient to take in a deep breath. At the peak of inspiration, apply a slow (approximately 2 times per second), rhythmic bouncing pressure to the chest wall until the end of expiration. The hands follow the movement of the chest as the air is exhaled. The frequency of shaking is 2 Hz.44,53
For shaking, with the patient in the appropriate PD position, place your hands over the lobe of the lung to be treated and instruct the patient to take in a deep breath. At the peak of inspiration, apply a slow (approximately 2 times per second), rhythmic bouncing pressure to the chest wall until the end of expiration. The hands follow the movement of the chest as the air is exhaled. The frequency of shaking is 2 Hz.44,53
Manual Hyperinflation
Airway Clearance Techniques