performed with the catheter in this position. If the case proceeds to carotid stent placement, the elbow or secondary curve of the catheter must be advanced into the artery at its origin to obtain exchange guidewire access to the common carotid artery. Carotid artery catheterization is discussed in more detail below.
Table 29-1 Skills Required for Carotid Angioplasty and Stenting | ||||||
|---|---|---|---|---|---|---|
|
not become inadvertently dislodged into the carotid bulb with breathing or arterial pulsation. The external carotid artery is roadmapped, and the best branch for anchoring the carotid sheath is chosen. The guidewire is advanced into the distal external carotid artery branch and is followed by the catheter. The Glidewire is subsequently removed. The selective cerebral catheter must be back bled to avoid introducing air into the system. This often requires withdrawing the catheter slightly, because its tip usually enters a small, distal branch. The exchange guidewire is then placed in the external carotid artery. Commonly used exchange guidewires are the Amplatz super-stiff (Cook, Inc., Bloomington, IN) or extra-stiff (Boston Scientific), the Supracore (Guidant, Menlo Park, CA), the Microvena Nitinol (Microvena Corp., White Bear Lake, MN), or a Stiff Glidewire (Boston Scientific). A braided, selective catheter is useful when advancing the stiff exchange guidewire into the external carotid artery, because it is less likely to be pulled out. After the exchange guidewire has been placed, the selective catheter is removed and the long, carotid guiding sheath is inserted. The guidewire is surveyed with fluoroscopy to look for any redundant segments; these should be removed before sheath passage. The 6 Fr sheath is commonly used with popular ones, including the Shuttle Sheath (Cook), Destination (Boston Scientific), and Vista Brite Tip (Cordis Corp., Miami Lakes, FL). The sheath is advanced over the exchange guidewire with steady forward pressure. The field of view should include the guidewire tip and the course of the guidewire from the arch into the common carotid artery to make certain that the guidewire is not migrating caudally. When the sheath tip reaches the last major turn from the arch into the common carotid artery, the angle of approach can be made less acute by having the patient take a deep breath.
 Figure 29-1. Normal versus elongated arch. A: This configuration of the aortic arch is relatively “normal.” B: This arch aortogram demonstrates elongation of the ascending and transverse aortic segments in an elderly hypertensive man. The junction of the distal arch and the proximal descending aorta comes to a peak where the aorta is “fixed” in the posterior mediastinum. The arch branches originate along its “up slope.” |
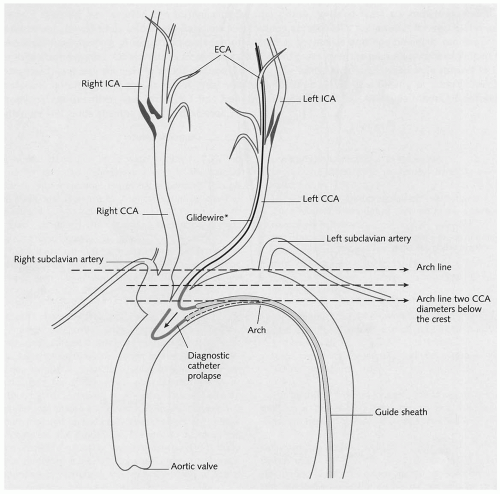 Figure 29-2. The diagram shows the designation of the arch levels 1, 2, or 3. A horizontal line is drawn across the “top” of the arch. The level 1 arch has branches originating along that line, from the “top” of the arch. The level 2 arch has branches originating more than one common carotid artery diameter caudal to the “top” of the arch. The level 3 arch has its branches originating more than two common carotid artery diameters caudal to the “top” of the arch. (Reproduced with permission from Myla S. Carotid access techniques: an algorithmic approach. Carotid Interv. 2001;3:2-12.) |
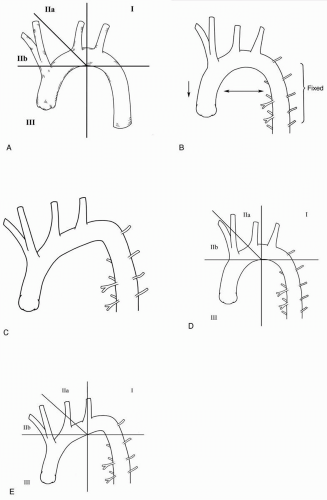 Figure 29-3. Aortic arch classification using the “surf and turf” classification. A: A horizontal line is drawn across the peak of the inner curve of the arch. This point forms a fulcrum and is the location over which the catheters must work to achieve carotid access. A vertical line is drawn at the location where the arch peaks superiorly. An additional line bisects the angle formed between these horizontal and vertical lines, thereby dividing the arch segments into I, IIa, IIb, and III regions. The further caudally and toward the patient’s right-hand side the branch vessels originate, the more challenging they are to catheterize and achieve sheath access. B: Normal arch. C: Elongated arch that “pushes” the origins of the branch vessels down into the chest and causes more acute curvature of the distal arch. This is representative of elderly patients with long-standing hypertension. D: When the “surf and turf” classification is applied to the normal arch, the left common carotid artery is in segment IIa, and the innominate and right common carotid artery are in segment IIb. E: The “surf and turf” classification applied to the elongated arch shows that the innominate and right common carotid arteries originate in segment III. (Reproduced with permission from Schneider PA. Carotid arteriography. In: Schneider PA, Bohannon WT, Silva MB Jr, eds. Carotid Interventions. New York: Marcel Dekker Inc, 2004:36.) |
and the lower profile. The main disadvantage of the monorail system is that it must be delivered directly into the side branch through a long sheath (rather than over a large-caliber guidewire). There is a learning curve associated with its use, but experienced vascular specialists consider it easier and faster than the standard coaxial system.
Table 29-2 Pitfalls Associated with Remote Access and Working Through a Long Sheath | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
The refinement of its accuracy to determine the degree of stenosis
The benefits of the arteriogram, in terms of reducing the complication rates of the open repair, do not outweigh its small risk
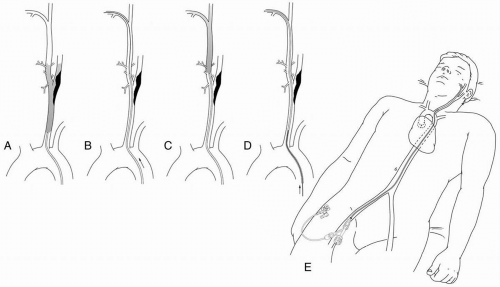 Figure 29-4. Placement of the sheath is illustrated. A: The common carotid artery is catheterized with a selective catheter, and a roadmap of the carotid bifurcation is obtained with the image intensifier rotated in such a way that the bifurcation is “opened up” or splayed out. B: A steerable guidewire is advanced into the external carotid artery, and the selective catheter is advanced over it. C: The selective catheter is used to perform a roadmap of the external carotid artery, and a long branch of the external carotid artery is chosen to anchor the stiff guidewire. D: The selective catheter is advanced into the distal segment of the external carotid artery branch, and a stiff exchange guidewire is placed. E: The short femoral access sheath is removed, and a long carotid guiding sheath is placed with its tip in the common carotid artery. (Reproduced with permission from Schneider PA. Access for carotid interventions. In: Schneider PA, Bohannon WT, Silva MB Jr, eds. Carotid Interventions. New York: Marcel Dekker Inc, 2004:100-102.) |
sheath is directed toward the surgeon, and pressure is maintained at the arteriotomy with the nondominant hand until the sheath enters the artery.
Table 29-3 Comparison of Coaxial and Monorail Systems | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 29-4 Current Indications for Carotid Arteriography for Extracranial Carotid Artery Occlusive Disease | ||||
|---|---|---|---|---|
|



