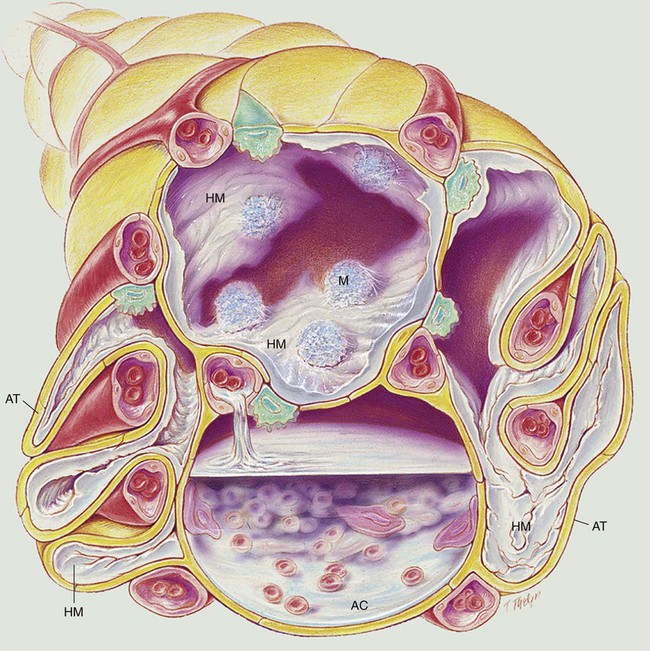
After reading this chapter, you will be able to: • List the anatomic alterations of the lungs associated with acute respiratory distress syndrome. • Describe the causes of acute respiratory distress syndrome. • List the cardiopulmonary clinical manifestations associated with acute respiratory distress syndrome. • Describe the general management of acute respiratory distress syndrome. • Describe the clinical strategies and rationales of the SOAPs presented in the case study. • Define key terms and complete self-assessment questions at the end of the chapter and on Evolve. In gross appearance the lungs of patients with ARDS are heavy and “red,” “beefy,” or “liver-like.” The anatomic alterations that develop in ARDS create a restrictive lung disorder (see Figure 27-1). The major pathologic or structural changes associated with ARDS are as follows: • Interstitial and intra-alveolar edema and hemorrhage • Intraalveolar hyaline membrane formation • Pulmonary surfactant deficiency or abnormality Historically, ARDS was first referred to as the “shock lung syndrome” when the disease was first identified in combat casualties during World War II. Since that time, the disease has appeared in the medical literature under many different names, all based on the conditions believed to be responsible for the disease. In 1967 the disease was first described as a specific entity, and the term acute respiratory distress syndrome was suggested. This term is predominantly used today. Box 27-1 provides some of the other names that have appeared in the medical journals to identify ARDS. A multitude of causative factors may produce ARDS. Box 27-2 provides some of the better-known causes. The following clinical manifestations result from the pathologic mechanisms caused (or activated) by Atelectasis (see Figure 9-9), Alveolar Consolidation (see Figure 9-9), and Increased Alveolar-Capillary Membrane Thickness (see Figure 9-10)—the major anatomic alterations of the lungs associated with ARDS (see Figure 27-1). CLINICAL DATA OBTAINED AT THE PATIENT’S BEDSIDE
Acute Respiratory Distress Syndrome
Anatomic Alterations of the Lungs
Etiology and Epidemiology
 OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Acute Respiratory Distress Syndrome
OVERVIEW of the Cardiopulmonary Clinical Manifestations Associated with Acute Respiratory Distress Syndrome