Fig. 14.1
Chest radiograph showing a large pleural-based mass in the left hemithorax (arrows), with underlying rib destruction and a pleural effusion (From Lim et al. [9] This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited)

Fig. 14.2
A contrast enhanced CT examination of the chest showing a large heterogenously enhancing solid mass arising from the skeletal chest wall with lytic destruction of the rib and calcifications (arrows). There is a moderate-sized pleural effusion (block arrow) and underlying lung collapse and consolidation (star) (From Lim et al. [9] This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited)
Most common benign chest wall tumors in infants and children are lymphangiomas, hemangiomas and mixed lymphangiohemangiomas. These often cystic tumors are typically located within the chest wall, axilla or neck and can increase rapidly in size due to spontaneous intracapsular hemorrhage. Benign soft tissue tumors affecting the thoracic wall during infancy and childhood are lipoblastoma, neurofibromatosis and fibrous tumors (fibroma, fibromatosis, fibrous hamartoma). Ribs, vertebrae, clavicle, scapula and sternum can be affected by osteochondromas as solitary or multiple lesions. Neurogenic chest wall tumors (schwannomas, neurofibromas) arise from intercostal nerves or sympatic ganglia and may lead to destruction of adjacent rips or vertebrae [5].
The majority of chest wall neoplasms in the adult patient population are malignant metastatic disease from either distant carcinomas or sarcomas, or due to direct invasion from adjacent thoracic malignancies of lung, pleura, mediastinum or breast [10].
Primary malignant chest wall tumors are rare findings, representing only 1–2 % of all primary tumors [11] and account for less than 1/3 of all chest wall neoplasms in the adult. The chest wall chondrosarcoma is the most common primary thoracic wall tumor, typically located in the anterior chest wall, arising parasternal from the costochondral junction or the sternum itself [12]. Osteosarcomas of the chest wall are rare. Although the osteosarcoma is the most common primary malignant tumor of the bone, only 3 % originate from the chest wall [13]. Ewing’s sarcomas are typically found in children, however 1/3 of cases encountered, affect patients above the age of 20 years. Further primary chest wall tumors reported in adult patients are plasmacytoma, soft tissue sarcoma and lymphoma. Radiation associated malignancies of the chest wall (malignant fibrous histiocytoma, radiation-induced sarcomas) may develop regardless of the original primary tumor and should be treated as de novo tumor [14].
Due to the rarity of primary chest wall tumors, most series published are of limited case numbers. Primary benign chest wall tumors have been reported to account for 21–67 % in various studies [10]. Osteochondroma and chondromas are the most common benign tumors. Lipoma is the most common benign soft tissue tumor. Benign tumors may cause significant chest wall deformities due to mass effect [15].
Iatrogenic Chest Wall Deformities
Iatrogenic deformities of the chest wall represent malformations which develop secondarily following a surgical intervention to the chest wall such as open repair of congenital pectus deformities, harvesting of rip grafts or inadequate closure of thoracotomies.
Surgical correction of pectus excavatum deformities involved originally various degrees of rip and cartilage resection. First surgical repair, with partial unilateral resection of 2nd and 3rd rip segments, was reported in 1911 by Ludwig Meyer [16]. His patient, however, suffered early recurrence of the deformity and associated respiratory symptoms [17]. Sauerbruch undertook in 1913 the first successful surgical repair of a pectus excavatum with satisfactory long-term result, performing a more extensive unilateral chondrocostal resection of the 5th to 9th rip with partial sternectomy [18]. The principle foundation of pectus surgery, on which all later on developed surgical techniques have orientated on, is attributed to Lexer and Hofmeister, who described in 1927 a technique of pectus excavatum repair involving bilateral chondrocostal resection with mobilization of the sternum [17]. This technique was developed further by Ravitch and published in 1949 [19]. The Ravitch procedure requires the excision of all deformed costal cartilages including pericondrium. Modifications of the Ravitch technique were reported by Welch and Shamberger [20, 21] and Robicsek [22–24] and remain basis for current open repair of the pectus excavatum deformity (Fig. 14.3a–c).
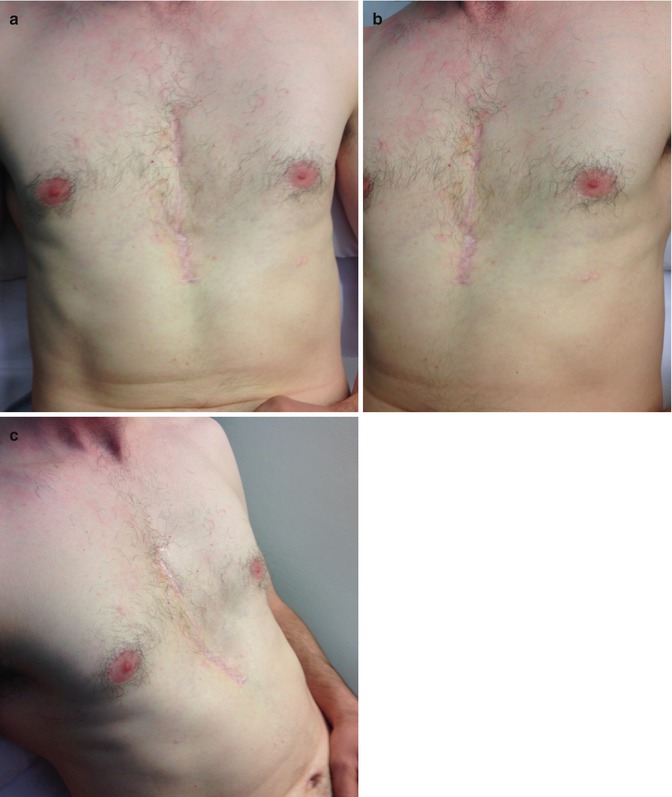
Fig. 14.3
(a) Sternal depression after Ravitch procedure; (b) Sternal depression after Ravitch procedure left side view; (c) Sternal depression after Ravitch procedure right side view
During the early and mid 1990s, the attention of the surgical society was directed at a group of young patients who presented with symptoms of severe respiratory distress during minimal exercise and universal physical finding of a small and narrow thorax with immobile chest wall and primary diaphragmatic breathing [25, 26]. All these patients, typically children and teenagers were in common a past medical history of extensive open repair of a pectus excavatum deformity during early childhood before the age of 4 years. None of the patients showed recurrence of the pectus deformity, however all had developed a reduced and restricted thorax with debilitating restrictive pulmonary disorder. Pulmonary function showed significantly decreased vital capacity and forced expiratory volume with impaired exercise capacity and desaturations during exercise [25, 26]. A history of recurrent episodes of pneumonia requiring hospitalization was common. Radiographic imaging identified markedly reduced sagittal and transverse diameters of the chest with low-lying diaphragm [1, 26]. The sternum was often atrophic, short and depressed. Para-sternal fusion of rips was common finding [27]. This restrictive chest wall condition following pectus repair was termed “acquired Jeune’s syndrome” due to the striking similarity of findings with the asphyxiating thoracic chondrodystrophy or Jeune’s syndrome [25]. Jeuen’s syndrome is a rare autosomal recessive disorder affecting the development of bone and cartilage with subsequent skeletal dysplasia [28]. Thoracic cage growth retardation with pulmonary hypoplasia leads frequently to death during infancy due to respiratory insufficiency. With improved postnatal management, patients may survive to childhood or early adolescence [29]. As the complex of Jeune’s syndrome extends beyond the chest wall anatomy, Robicsek introduced the term of “acquired restrictive thoracic dystrophy” (ARTD) to describe the complication of a restricted and dystrophic chest cage following extensive pectus excavatum deformity repair [30]. A uniform terminology has not yet been agreed on. Authors continue to use multiple terms, such as “acquired restrictive thoracic dystrophy (ARTD)” [30], “acquired asphyxiating thoracic dystrophy [31, 32], “acquired thoracic dystrophy” [33] or “acquired Jeune’s syndrome” [27].
Thoracic growth retardation in ARTD is a direct result of surgical trauma to the costochondral growth plates or of their resection at young age, with the degree of ARDT severity depending upon the extent of cartilage extirpation [1]. Injury or resection of the costochondral growth centers prevents normal development and growth of the rip cage. Experimental studies have identified the sternal costochondral junction as the site where most of the longitudinal growth of the rib takes place as a result of endochondrial bone formation [34, 35]. During infancy, when compared to childhood, a significantly higher number of cells and proportion of proliferative chondrocytes are present at the sternal costochondral junction [36]. Excision of costal cartilages without preservation of the costal growth centers severely affects the transvers and sagittal thoracic development as shown in experimental studies by Martinez et al. [37] and Calik et al. [38]. In addition, further restriction of the chest can be caused by retrosternal suturing of rips or perichondral sheaths as additional sternal support, a technique introduced during the 1970s as adjunctive maneuver to prevent recurrence of sternal depression [39]. However, fibrosis and cartilage regeneration with subsequent ossification leads to formation of restrictive and fixed sub sternal plane, resulting in a frozen thorax [40]. Not only thoracic growth retardation with reduction in size, but also a severely impaired mobility and fixation of the chest wall is responsible for the observed cardiopulmonary effects in ARTD patients [25, 33].
The treatment of the acquired Jeune’s syndrome remains a surgical challenge and is aimed to improve functional lung capacity by increasing the overall thoracic volume. A low-lying diaphragm and predominant diaphragmatic breathing are common findings. Improvement of pulmonary function may be achieved by enlargement of the thoracic cage with subsequent improved diaphragmatic respiration. Extensive and aggressive reconstruction of the chest wall is required in most cases. Reconstructive techniques in children often require multiple and staged procedures to enable progressive expansion of the chest during the child’s growth. A number of techniques have been described. Due to the rarity of the condition, the published series consist of limited number of cases and further modifications of surgical techniques and strategies are to be expected.
In his landmark report on restrictive thoracic dystrophy following corrective pectus surgery at early age, which was the first report of its kind, Haller described during his presentation in 1995 a technique of anterior chest wall enlargement consisting of sternal mobilization with resection of the degenerated fibro-osseous sternocostal junction. The sternum was then elevated and fixed using multiple modified Rehbein splints [25].
Surgical experience gained in the treatment of the congenital Jeune’s syndrome was transferred into the operative management of the acquired Jeune’s syndrome. Barnes and Hull, surgeons at London’s Great Ormond Street Hospital described in 1971 a technique of thoracic volume enlargement for children with congenital Jeune’s syndrome, involving a median sternotomy and splinting of the sternum using autologous bone graft and bone matrix [41]. This surgical technique has since been refined and recommended for its simplicity, short operating time, and effectiveness [42, 43]. At the St Louis’ Cardinal Glennon Children’s Hospital, Weber adopted Barnes’ technique for his ARTD patients. Weber and colleagues reported in 1998 their first case of ARTD correction using the technique of sternal midline split with permanent separation of the sternal halves by rip graft interposition [31]. Additional rib cage enlargement was achieved by bilateral rip resection. In 2005, Weber’s group published a further report on a total of ten patients treated by the method described above with overall satisfactory functional results [32].
In 2014, Paul Colombani’s group of the John Hopkins Hospital published their experience and surgical approach [27]. Between 1996 and 2011, 19 patients (aged 11–37 years) underwent extensive chest wall reconstruction for ARTD following Ravitch procedure at a mean age of 4.63 years. Sufficient re-expansion of the chest cage was achieved by repeated modified Ravitch procedure in two patients. The remaining 17 patients required extensive reconstructive surgery to achieve expansion of the thoracic cage by mobilization and elevation of the sternum and complete reconstruction of the anterior chest wall. Thorough exposure of the anterior thoracic cage was achieved by mobilization of bilateral pectoralis muscle flaps and separation of the rectus abdominis muscle from the xyphoid through a transvers anterior chest wall incision. Mobilization of the sternum was achieved by bilateral transection of the parasternal fibrous scar tissue and resection of deformed cartilages. A transvers anterior osteotomy at the sterno-manubrial junction was made to allow elevation of the corpus sterni by wiring the corpus onto the top edge of the manubrium. The costosternal continuity was restored by wiring of the lower cartilages to the sternum to improve stability of the anterior chest wall. Reconstruction of the costosternal margin in the absence of cartilages required utilization of autologous rip graft or femur allograft. Bilateral thoracic expansion gaps were created by serial rip osteotomies to allow further release of the anterior chest wall. One or two Lorenz bars were placed for retrosternal support.
A similar surgical technique, applied to adult ARTD patients, was reported in 2014 by Jaroszewski and co-workers from the Mayo Clinic Hospital in Phoenix [33]. Their patient collective consisted of nine male patients with a mean age of 34 years (range 22–42 years), who all underwent a Ravitch procedure for correction of pectus excavatum deformity between their 4th and 6th year of life. The operative approach involved the full mobilization of the sternum with multiple parasternal and lateral rip osteotomies to allow for anterior expansion of the thoracic cage and elevation of the sternum. Sternal support was provided with a Lorenz bar. Multiple Titanium plates were used to stabilize the sternal osteotomy and lateral chest wall. The sternocostal junctions were reconstructed using Polyglactin mesh and bone matrix.
Operative and functional outcome of ARTD surgery are encouraging. Although the chest wall reconstructions are complex procedures with significant potential intra- and postoperative complications, a successful repair can be performed safely. The majority of patients reported a subjective improvement in preoperative symptoms, ability to exercise and quality of life [27, 32, 33]. Postoperative improvement of measurable pulmonary function is however modest only [27], emphasizing the severity of permanent thoracic organ dysfunction due to persistent limitation of thoracic wall excursion and ceased growth development caused by the condition.
Prevention of ARTD as complication of corrective pectus surgery is adamant. All reported patients suffering from ARTD underwent a Ravitch-type operation at a very young age. It was therefore quickly advocated that open surgical correction of a pectus deformity should be delayed until skeletal growth and development are completed. However, Robicsek argued that pectus surgery can be performed safely even at young age as long the essential principle of limited cartilagous resection ensuring preservation of the costochondral growth centres in not violated [22, 30]. A segment of cartilage should be preserved at the sternal and costal end. The posterior perichondrium should be preserved in its entire length to allow for chondral regeneration. Retrosternal suturing of perichondrium or rips must be avoided as this manoeuvre has been shown to contribute significantly to thoracic constriction due to fibrosis and ossification. Robicsek concluded that “the solution to the problem of preventing the development of acquired restrictive thoracic dystrophy after pectus excavatum repair is not to delay surgical intervention, but to do it appropriately.” [1]
Other forms of iatrogenic chest wall malformations are pectus deformities, which develop after surgical intervention involving the sternum or anterior chest wall. Most common are acquired pectus carinatum deformities, evolving several years postoperatively [44, 45]. The initial surgery often over-corrected an existing pectus excavatum deformity. Development of an iatrogenic pectus carinatum has also been observed following median sternotomy for cardiac surgery in early childhood [46]. A carinatum-type deformity has been reported after corrective surgery for sternal cleft malformation [45]. The “floating sternum” describes an unstable anterior chest wall with chronic and persistent complete detachment of the sternum from all costochondral junctions [40]. This complication of pectus excavatum repair has been observed years after the initial surgery and is understood to be caused by extensive resection of the costal cartilages and perichondrium or failure of proper regeneration of resected cartilages [47].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


