Contrast-induced nephropathy (CIN) is associated with increased morbidity and mortality rates. Although a previous study reported that pretreatment with sodium bicarbonate is more effective than sodium chloride for prophylaxis of CIN, this has not been a universal finding. We performed a prospective randomized trial to investigate whether CIN can be avoided using sodium bicarbonate. In total 155 patients with a glomerular filtration rate (GFR) <60 ml/min/1.73 m 2 who were undergoing coronary angiography were enrolled. We assigned patients to sodium chloride plus sodium bicarbonate (bicarbonate group, n = 78) or sodium chloride alone (chloride group, n = 77). Infusion of sodium bicarbonate at 1 ml/kg/hour continued from 3 hours before to 6 hours after coronary angiography. CIN was defined as a 25% increase in serum creatinine from baseline value or an absolute increase of ≥0.5 mg/dl, which appeared within 2 days of contrast. Baseline GFR was not significantly different between the 2 groups. Patients in the bicarbonate group had a higher GFR than those in the chloride group on day 2 (45.8 ± 13.4 vs 40.9 ± 14.6 ml/min/1.73 m 2 , p = 0.031) and at 1 month (49.5 ± 14.7 vs 43.7 ± 15.5 ml/min/1.73 m 2 , p = 0.019). CIN occurred in 10 patients (13%) in the chloride group but in only 2 patients (2.6%) in the bicarbonate group (p = 0.012). Sodium chloride plus sodium bicarbonate is more effective than sodium chloride alone for prophylaxis of CIN and can lead to retention of better long-term renal function.
Reactive oxygen species have an important role in the pathogenesis of contrast-induced nephropathy (CIN). In animal studies, superoxide dismutase, a scavenger of reactive oxygen species, prevented renal damage by contrast agents. The reported benefit of the free radical scavenger N -acetylcysteine supports the hypothesis that CIN is caused by free radical generation. Sodium bicarbonate has antioxidant effects and scavenges reactive free radicals. Recent studies have reported that hydration with sodium bicarbonate is more effective than with sodium chloride. However, contradictory results regarding the efficacy of sodium bicarbonate have been reported, and the protective effect of sodium bicarbonate is equivocal. In addition, the effect of prophylactic sodium bicarbonate on renal function over the long term is unknown. To fill these gaps in knowledge, we conducted a prospective, randomized, multicenter, open-labeled trial to test the hypothesis that infusion of sodium bicarbonate plus sodium chloride would be more effective at inhibiting CIN in patients with chronic kidney dysfunction undergoing planned coronary angiography or intervention than infusion of sodium chloride alone. In addition, we hypothesized that infusion of sodium bicarbonate would prevent CIN and have a long-term benefit in renal function.
Methods
We prospectively enrolled patients undergoing coronary angiography or intervention at 2 Japanese hospitals from November 2004 through May 2007. Indications for coronary angiography or intervention for each patient were left to the discretion of each clinical cardiologist. All patients were ≥20 years old and had an estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m 2 . Exclusion criteria included serum creatinine levels >4 mg/dl, changes in serum creatinine levels of ≥0.5 mg/dl during the previous 24 hours, pre-existing dialysis, pulmonary edema, uncontrolled hypertension (treated systolic blood pressure >160 mm Hg or diastolic blood pressure >100 mm Hg), emergency catheterization, exposure to radiographic contrast within previous 2 days, and any allergy to radiographic contrast medium. No patients received any treatment that influenced renal function including dopamine, mannitol, fenoldopam, or N -acetylcysteine during the intended period of the study.
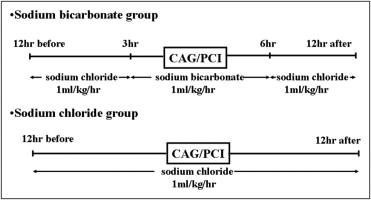
Patients were randomly assigned to receive sodium bicarbonate plus sodium chloride (bicarbonate group) or sodium chloride alone (sodium chloride group) based on random numbers generated by computer. All patients received 0.9% sodium chloride for 12 hours before and after the procedure. The sodium bicarbonate solution was prepared by adding 154 ml of sodium bicarbonate 1,000 mEq/L to 846 ml of 5% dextrose in water. In the sodium bicarbonate group the sodium bicarbonate solution was changed 3 hours before contrast administration ( Figure 1 shows treatment schedule).
Echocardiographic evaluation of left ventricular function was performed in all patients on admission. The nonionic, low-osmolality contrast medium, iopamidol (Isovue, Bracco Diagnostics, Inc., Princeton, New Jersey) was used in all cases. Diuretics were stopped 24 hours before contrast administration and restarted only when renal function had been shown to be stable after the procedure.
Serum creatinine concentration was assessed at time of hospital admission and on days 1 and 2 and at 1 month after the procedure. eGFR obtained using a model excluding urine biochemistry values was calculated at time of hospital admission and on days 1 and 2 and at 1 month after the procedure. All tests were performed in the hospital-based laboratory with consistent methods. Data were recorded in a dedicated database. The study protocol was approved by the local ethics committee and all patients gave written informed consent.
The primary end point of the study was development of CIN, defined as a 25% increase or an absolute increase of ≥0.5 mg/dl in serum creatinine from baseline value, which appeared within 2 days of the produce. Additional end points were (1) change in serum creatinine and eGFR calculated on days 1 and 2 and (2) long-term renal function assessed 1 month after the procedure.
The sample size was selected to demonstrate a decrease in the primary end point of CIN from 15% in the chloride group to 2% in the bicarbonate group. Using Fisher’s exact probability test with a significance level of 0.05, 158 randomized patients were calculated to give the study 90% power.
Analysis was conducted on an intention-to-treat basis. Categorical variables such as incidence of CIN were analyzed by Fisher’s exact test. Differences between groups were analyzed by nonparametric Wilcoxon–Mann–Whitney test. Analyses were performed with StatView 5.0 (SAS Institute, Cary, North Carolina). All statistical tests were 2-sided and a p value <0.05 was considered statistically significant.
Results
In total 158 patients were randomized to receive sodium bicarbonate plus sodium chloride (n = 79) or sodium chloride (n = 79), with 155 patients completing the study. Of the 158 patients, 3 did not complete the study. Two patients in the chloride group had no follow-up laboratory test results. In the bicarbonate group, 1 patient had to interrupt the infusion of sodium bicarbonate because of angialgia.
Clinical characteristics of the 155 patients who completed the study are listed in Table 1 . There were no significant differences between groups with regard to age, gender, or incidence of diabetes mellitus. No significant differences in baseline procedural characteristics were found between the 2 groups. Urine pH measurements before procedures confirmed that patients receiving sodium bicarbonate developed urinary alkalinization ( Table 2 ). In addition, as expected, a significant increase in serum bicarbonate occurred in patients receiving sodium bicarbonate. There was a small but not significant decrease in serum potassium in the bicarbonate group, indicating that the alkaline load from sodium bicarbonate did not induce a decrease in serum potassium sufficient to create a risk for disturbances of cardiac rhythm.
| Characteristics | Bicarbonate Group (n = 78) | Chloride Group (n = 77) |
|---|---|---|
| Age (years) | 71 ± 9 | 74 ± 7 |
| Men | 59 (76%) | 49 (64%) |
| Weight (kg) | 61 ± 11 | 63 ± 10 |
| Smoking | 48 (61%) | 37 (48%) |
| Diabetes mellitus | 44 (56%) | 49 (63%) |
| Hypertension | 67 (86%) | 64 (83%) |
| Hyperlipidemia | 38 (48%) | 42 (54%) |
| Old myocardial infarction | 30 (38%) | 25 (32%) |
| Angiotensin-converting enzyme inhibitor or angiotensin receptor blocker | 62 (79%) | 69 (90%) |
| Cardiac catheterization | 44 (56%) | 36 (47%) |
| Percutaneous coronary intervention | 34 (44%) | 41 (53%) |
| Target coronary lesion | ||
| Left anterior descending coronary artery | 13 (17%) | 15 (19%) |
| Left circumflex coronary artery | 8 (10%) | 12 (16%) |
| Right coronary artery | 13 (17%) | 14 (18%) |
| Ejection fraction (%) | 57 ± 11 | 53 ± 15 |
| Contrast volume (ml) | 140 ± 50 | 130 ± 40 |
| Characteristics | Bicarbonate Group (n = 78) | Chloride Group (n = 77) | P Value |
|---|---|---|---|
| Baseline urine pH | 5.69 ± 0.97 | 5.84 ± 0.82 | 0.33 |
| Baseline serum creatinine (mg/dl) | 1.54 ± 0.43 | 1.55 ± 0.44 | 0.81 |
| Baseline estimate glomerular filtration rate (ml/min/1.73 m 2 ) | 45.7 ± 12.9 | 42.8 ± 13.8 | 0.18 |
| Baseline serum potassium (mEq/dl) | 4.40 ± 0.73 | 4.49 ± 0.44 | 0.37 |
| Baseline serum bicarbonate (mEq/dl) | 24.23 ± 1.94 | 24.85 ± 1.99 | 0.073 |
| Urine pH immediately before procedure | 6.36 ± 1.14 | 5.83 ± 0.75 | <0.01 |
| Change in serum potassium (mEq/L) | −0.46 ± 0.61 | −0.32 ± 0.38 | 0.098 |
| Change in serum bicarbonate (mEq/L) | 1.87 ± 1.43 | 0.12 ± 1.24 | <0.01 |
Mean serum creatinine for all patients was 1.54 ± 0.43 mg/dl. Regarding serum creatinine levels ( Table 3 ), the bicarbonate group tended to have a lower level than the chloride group on day 1, day 2, and 1 month after the procedure. In the chloride group, mean serum creatinine increased from baseline on day 1, day 2, and at 1 month (p = 0.41, 0.0011, and 0.071 respectively) after contrast administration. In the bicarbonate group, mean serum creatinine level decreased significantly from baseline on day 1 and 1 month after contrast administration (p = 0.027 and 0.0023, respectively).
| Characteristics | Bicarbonate Group (n = 78) | Chloride Group (n = 77) | p Value |
|---|---|---|---|
| Baseline serum creatinine (mg/dl) | 1.54 ± 0.43 | 1.55 ± 0.44 | 0.81 |
| Serum creatinine at day 1 (mg/dl) | 1.49 ± 0.43 | 1.57 ± 0.42 | 0.26 |
| Serum creatinine at day 2 (mg/dl) | 1.56 ± 0.46 | 1.66 ± 0.54 | 0.23 |
| Serum creatinine at 1 month (mg/dl) | 1.46 ± 0.43 | 1.60 ± 0.49 | 0.054 |
| Baseline estimated glomerular filtration rate (ml/min/1.73 m 2 ) | 45.7 ± 12.9 | 42.8 ± 13.8 | 0.18 |
| Estimated glomerular filtration rate at day 1 (ml/min/1.73 m 2 ) | 47.2 ± 12.7 | 42.3 ± 14.2 | 0.025 |
| Estimated glomerular filtration rate at day 2 (ml/min/1.73 m 2 ) | 45.8 ± 13.4 | 40.9 ± 14.6 | 0.031 |
| Estimated glomerular filtration rate at 1 month (ml/min/1.73 m 2 ) | 49.5 ± 14.7 | 43.7 ± 15.5 | 0.019 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


