A family with asymptomatic Wenckebach atrioventricular block (Wenckebach periodicity [WP]) has been followed at the investigators’ institution for >4 decades. In contrast to all reported cases of WP (except in top-ranking athletes) family members have WP at rest that promptly converts to regular sinus tachycardia with exercise. They also have mild apical noncompaction that has been quite stable. Because of apparent autosomal dominant inheritance of the structural and arrhythmia disorders, deoxyribonucleic acid was obtained from 4 affected family members in 2 generations for sequence analysis of the cardiac transcription factor gene NKX2.5. A novel frame-shift mutation (c.959delC) was identified that would result in premature truncation of the protein at residue 293, with loss of the C-terminal 31 amino acids. The responsiveness of WP to exercise, the long-term stability of the WP rhythm, and the mild asymptomatic structural features expand the phenotypic presentation of diseases related to mutations in NKX2.5. In addition, the physiology of WP is reviewed in these subjects and in highly conditioned athletes. In conclusion, the investigators report familial stable WP and ventricular noncompaction caused by a mutation in NKX2.5.
In the course of following a multigenerational family for >40 years, we observed an unusual combination of Wenckebach arrhythmia and mild noncompaction of the left ventricle in several members, suggesting an inherited disorder. Wenckebach periodicity (WP) is almost always a manifestation of the atrioventricular (AV) node (nodal conduction). WP can occur in patients with intrinsic AV nodal disease, myocarditis, acute inferior myocardial infarction or ischemia, and cardiac surgery and in those who are taking drugs that block the AV node. It can also occur in highly conditioned athletes as a consequence of high vagal tone, in which it manifests in association with a normal heart rate and disappears with exercise-induced tachycardia. The occurrence of structural and rhythm disturbances in this family suggested that their disease might be caused by a mutation in the cardiac homeobox gene, NKX2.5 (Online Mendelian Inheritance in Man 600584). This gene encodes a transcription factor that plays a crucial role in cardiogenesis. Among the more common manifestations of NKX2.5-related disease are septal defects and progressive AV nodal heart block. Herein, we describe a novel frame-shift mutation in NKX2.5 in our family responsible for the unusual, very stable WP that occurs in association with a normal heart rate and resolves with exercise-induced tachycardia.
Methods
Patients were evaluated and samples were collected from 4 patients in 2 generations under a protocol approved by the institutional review board of the University of Washington. Saliva samples were obtained in Oragene OG-500 kits (DNA Genotek, Inc., Kanata, Ontario, Canada), and deoxyribonucleic acid was extracted per the direction of the manufacturer. Genomic deoxyribonucleic acid was extracted from blood using standard procedures. The 2 exons of NKX2.5 were amplified by polymerase chain reaction in an MJ Research DNA Engine Tetrad 2 (Bio-Rad Laboatories, Hercules, California) using the following primer sets given in 5′ to 3′ direction: 1.1 F TTTGCCGTATGACTATATTAGGTG and 1.1 R AGCATGCAGGAGGAGGG, 1.2 F CCCACGCCCTTCTCAGTC and 1.2 R AGGGCGCGTGTCTCCTC, 2.1 F CTCCACGAGGATCCCTTACC and 2.1 R ATAACCGTAGGGATTGAGGC, 2.2 F CTACAAGTGCAAGCGGCAG and 2.2 R GCCACAAACTCTCCCGTG, 2.3 F GACCCTGACCGATCCCAC and 2.3 R GGAATGCCTGTGCCTGAG, and 2.4 F GTGCTGAAACTCACGTCCAC and 2.4 R GCCGAAGTTCACGAAGTTGT. Sequencing was performed on an ABI 3130XL sequencer (Applied Biosystems, Foster City, California) using the same forward primers and ABI BigDye Dye Terminator v3.1 Cycle Sequencing kits (Applied Biosystems). Further analysis was performed with SeqScape version 2.1 (Applied Biosystems). The mutation in exon 2 was corroborated by sequencing using primer 2.4R.
Results
Clinical history
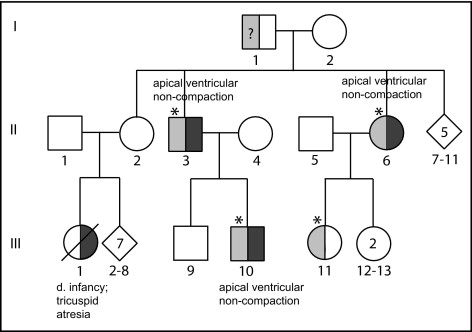
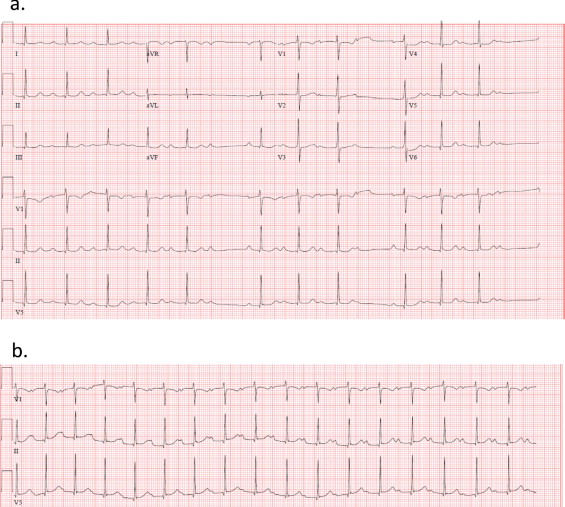
The pedigree is shown in Figure 1 . The proband, patient II-3, was first observed in 19 years of age, when he was hospitalized for a sport injury and, because of bradycardia, an electrocardiogram was recorded that revealed 2:1 AV block. With exercise, this converted to 1:1 conduction with sinus tachycardia. Subsequently, WP was documented at rest ( Figure 2 ). The proband is now 55 years old and has no cardiac symptoms except for episodic palpitations. He has normal exercise tolerance, but has been found on echocardiography to have mild apical noncompaction of the left ventricle, with an excellent ejection fraction. His 37-year-old son, patient III-10, also has persistent WP, noted since 7 years of age, and mild apical noncompaction of the left ventricle. The proband’s niece, patient III-11, is a 30-year-old woman who has occasionally had the sensation of intermittent heart fluttering since 21 years of age. She came to medical attention after syncope in the setting of phlebotomy, at which time WP was observed; she has not experienced recurrent syncope. As demonstrated in Figure 2 , her baseline rhythm shows WP with progressive prolongation of the PR interval, followed by dropped beat. WP resolves with adrenergic stimulation or minor exercise such as leg lifts, during which her heart rate increases and there is 1:1 conduction with first-degree AV block ( Figure 2 ). WP returns with rest. She has not undergone echocardiography. At 51 years of age, her mother, patient II-6, was found to have episodic WP during continuous telemetry monitoring as part of workup for possible sleep apnea. These episodes all occurred during sleep and were independent of apneic spells. Mild left ventricular-apical noncompaction was seen on echocardiography. A niece of the proband, patient III-1, reportedly died in infancy of tricuspid atresia. This branch of the family was unavailable for evaluation. Patient I-1 is an 82-year-old man with coronary artery disease who has undergone coronary artery bypass graft surgery. His affected children and grandchildren report that at rest, he has the same arrhythmia as described in them and that it normalizes with exercise.
NKX2.5 sequencing
The clinical features in this family strongly suggested that a mutation in NKX2.5 might be present. Targeted sequencing of its 2 exons revealed a 1-bp deletion (c.959delC) in exon 2 ( Figure 3 ). This predicts a premature termination at residue 293 (val) and truncation of 31 amino acids from the C terminus. No nucleotide variants were detected at this position, and only 1 amino acid–changing variant was detected within 50 bases upstream and downstream of the position in 4,208 Caucasian and 2,146 African American exomes annotated in the National Heart, Lung, and Blood Institute’s Exome Sequencing Project Exome Variant Server ( http://evs.gs.washington.edu/EVS/ ).

Results
Clinical history
The pedigree is shown in Figure 1 . The proband, patient II-3, was first observed in 19 years of age, when he was hospitalized for a sport injury and, because of bradycardia, an electrocardiogram was recorded that revealed 2:1 AV block. With exercise, this converted to 1:1 conduction with sinus tachycardia. Subsequently, WP was documented at rest ( Figure 2 ). The proband is now 55 years old and has no cardiac symptoms except for episodic palpitations. He has normal exercise tolerance, but has been found on echocardiography to have mild apical noncompaction of the left ventricle, with an excellent ejection fraction. His 37-year-old son, patient III-10, also has persistent WP, noted since 7 years of age, and mild apical noncompaction of the left ventricle. The proband’s niece, patient III-11, is a 30-year-old woman who has occasionally had the sensation of intermittent heart fluttering since 21 years of age. She came to medical attention after syncope in the setting of phlebotomy, at which time WP was observed; she has not experienced recurrent syncope. As demonstrated in Figure 2 , her baseline rhythm shows WP with progressive prolongation of the PR interval, followed by dropped beat. WP resolves with adrenergic stimulation or minor exercise such as leg lifts, during which her heart rate increases and there is 1:1 conduction with first-degree AV block ( Figure 2 ). WP returns with rest. She has not undergone echocardiography. At 51 years of age, her mother, patient II-6, was found to have episodic WP during continuous telemetry monitoring as part of workup for possible sleep apnea. These episodes all occurred during sleep and were independent of apneic spells. Mild left ventricular-apical noncompaction was seen on echocardiography. A niece of the proband, patient III-1, reportedly died in infancy of tricuspid atresia. This branch of the family was unavailable for evaluation. Patient I-1 is an 82-year-old man with coronary artery disease who has undergone coronary artery bypass graft surgery. His affected children and grandchildren report that at rest, he has the same arrhythmia as described in them and that it normalizes with exercise.



