The National Cholesterol Education Program Adult Treatment Panel (ATP) has provided education and guidance for decades on the management of hypercholesterolemia. Its third report (ATP III) was published 10 years ago, with a white paper update in 2004. There is a need for translation of more recent evidence into a revised guideline. To help address the significant challenges facing the ATP IV writing group, this statement aims to provide balanced recommendations that build on ATP III. The authors aim for simplicity to increase the likelihood of implementation in clinical practice. To move from ATP III to ATP IV, the authors recommend the following: (1) assess risk more accurately, (2) simplify the starting algorithm, (3) prioritize statin therapy, (4) relax the follow-up interval for repeat lipid testing, (5) designate <70 mg/dl as an “ideal” low-density lipoprotein cholesterol target, (6) endorse targets beyond low-density lipoprotein cholesterol, (7) refine therapeutic target levels to the equivalent population percentile, (8) remove misleading descriptors such as “borderline high,” and (9) make lifestyle messages simpler. In conclusion, the solutions offered in this statement represent ways to translate the totality of published reports into enhanced hyperlipidemia guidelines to better combat the devastating impact of hyperlipidemia on cardiovascular health.
The National Cholesterol Education Program (NCEP) Adult Treatment Panel (ATP) has provided education and guidance for decades on the management of hypercholesterolemia. Its third report (ATP III) was published 10 years ago, with a white paper update in 2004. We continue to wait intently while the ATP IV writing group works to translate more recent evidence into a revised guideline. As the French proverb goes, “People count up the faults of those who keep them waiting.” This statement identifies significant challenges in moving from ATP III to ATP IV and aims to help address these challenges by providing balanced recommendations. We aim for simplicity to increase the likelihood of implementation in clinical practice.
Recommendation 1: Assess Risk More Accurately
Matching therapeutic intensity to estimated cardiovascular risk optimally balances benefits and dose-dependent risks. ATP III recommends the Framingham risk score (FRS) to determine the 10-year risk for developing a myocardial infarction (MI) or death from coronary heart disease (CHD) on the basis of age, gender, total and high-density lipoprotein (HDL) cholesterol, smoking, and blood pressure (or antihypertensive treatment). However, this method limits the inputs (traditional risk factors only), outputs (point estimate risk for nonfatal MI and CHD death only), and time span (10 years only).
A 50-year-old woman with a total cholesterol level of 250 mg/dl, an HDL cholesterol level of 60 mg/dl, untreated systolic blood pressure of 160 mm Hg, and no diabetes or tobacco use is estimated to carry a 2% cardiovascular risk over the next 10 years. However, the ATP FRS end point ignores noncoronary forms of occlusive atherosclerotic vascular disease and also overlooks lifetime risk, which is actually about 50% in this woman. Moreover, ATP III views her risk as the same even if she has metabolic syndrome, stage 2 chronic kidney disease, a strong family history of premature CHD, or a coronary artery calcium score of 400. Although “ATP III recognizes that risk for CHD is influenced by other factors [that] can modulate clinical judgment,” these are not incorporated into the treatment algorithm. Unfortunately, most adults presenting with their first MIs were not considered candidates for statin therapy on the basis of their ATP III–predicted risk before having events.
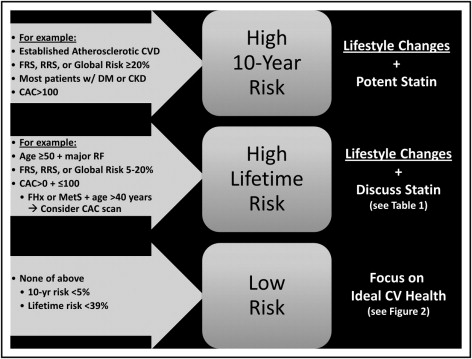
We recommend incorporating risk assessment tools beyond the ATP FRS into the treatment algorithm ( Figure 1 ) . More comprehensive risk assessment could enhance the efficiency of statin therapy allocation, optimize the risk/benefit ratio, and ensure that more patients who may benefit from therapy are not missed. Because statin trials did not randomize patients to treatment strategies on the basis of the ATP FRS, the scientific justification for this proposal is the same as for the Framingham tool itself: as estimated risk increases, more aggressive therapy provides greater absolute benefit.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


