Fig. 3.1
Mechanism of valve closure
In the upright posture, a reflux lasting less than 0.5 s is physiological; if the duration exceeds 0.5 s, it is defined as pathological reflux. The importance of incompetence of a single valve or several valves in genesis of clinical effects is not definitely known [2].
Muscle Pumps
The calf muscle pump is the most powerful force that facilitates venous return from the lower limbs. The thigh and foot muscle pumps also function to some extent toward this purpose.
Contraction of the calf muscle pump increases the pressure within the fascial compartments and forces blood up along the deep venous system (systole of the muscle pump). The competent valves prevent reflux distally within the deep venous system or through the perforators into the superficial veins (Fig. 3.2).
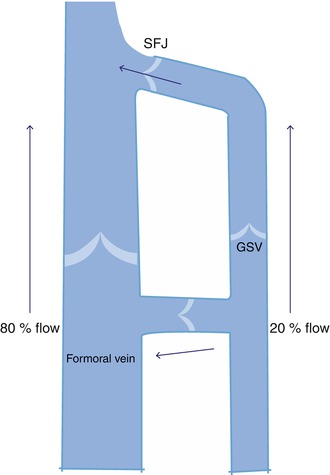
Fig. 3.2
Normal venous drainage of lower limb
When the calf muscles relax, the pressure in the fascial compartment drops. During this phase, blood from the superficial veins and the sinuses fills the deep system through the perforating veins (diastole of the muscle pump). The deep fascia of the leg supports the muscle pump considerably. The net effect of a series of contractions of the calf muscle pump would be to promote a streamlined, unidirectional, and cephalad flow toward the heart. This effectively reduces the pressure and volume in the superficial venous system during ambulation [3, 6].
The thigh muscle pump is not as powerful as the calf muscle pump in spite of the fact that these muscles are bulkier. Two reasons are attributed for its less powerful action – rapid refill and less compressible intermuscular location of the deep veins in the thigh [2]. The ejection fraction of the calf muscle pump is around 65 %, in comparison with only 15 % for the thigh pump [6].
The foot and lower leg biomechanics also play a major role in venous return. When the sole of the foot makes contact with the ground, the lateral plantar veins are emptied and blood is forced into the posterior tibial veins. This marks the first but essential step of venous return from the lower limbs. The calf muscle pump then sequentially takes over from the foot muscle pump [7]. When the foot muscle pump contracts, 50 % of the perforators of the foot permit flow from the deep to the superficial veins [2]. The role of the foot muscle pump could be crucial in the genesis of chronic venous disorders. It has been identified that static foot disorders may be associated with impaired venous return from the lower limbs [7].
In an average individual walking 100 steps a minute, the combined stroke volume of the calf muscle pumps of both sides is estimated as 6.0 l/min2.
Correlation with Ambulatory Venous Pressure Studies
In the clinical setting, the function of the calf muscle pump is best demonstrated by recording the ambulatory venous pressure (AVP) in the foot veins. AVP studies are primarily aimed at recording the drop in venous pressure in the superficial veins of the foot following a series of calf muscle contractions such as standing on toes [8].
A foot vein is cannulated and connected to a pressure transducer and a three-channel recorder or a manometer system through a three-way stopcock and a saline reservoir. The pressure in the foot vein with the patient standing upright and at rest is first recorded – resting pressure (RP). This will be roughly equivalent to the weight of the column of blood from the right heart to the point of measurement and varies according to the height of the individual. On an average, it is around 100 mm of Hg. The subject is asked to perform a series of standing on toe movements with the cannula in situ. This will produce a powerful contraction of the calf muscle. The pressure after a series of 10–15 contractions drops down by 50–60 % and thereafter remains steady irrespective of the extent of activity. The lowest pressure recorded after the series of muscle contractions is designated as the postexercise pressure (PEP). On cessation of the exercise, when the subject is at rest, the pressure slowly returns to the original resting value. The time taken for the PEP to return to the RP is designated as the recovery time (RT). In normal subjects, this is about 20–30 s. This AVP pattern is known as the normal venous pattern (Fig. 3.3).
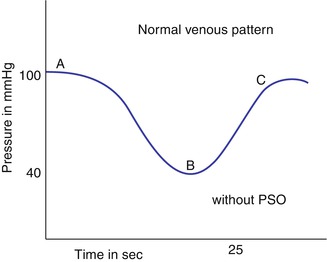
Fig. 3.3
AVP normal venous pattern. Note the prominent drop in PEP. (A) Resting pressure at start of exercise. (B) Maximum pressure fall with exercise. (BC) Recovery time
In patients with venous disorders, the drop in PEP is very negligible. Also, the recovery time is much faster (0–5 s). Thus the AVP pattern, normal and abnormal, can give an insight into the functioning of the calf muscle pump in health and disease.
Abnormal Hemodynamics in Chronic Venous Disorders
As we have seen in the previous section, the activity of the calf muscle pump reduces the pressure and volume of blood in the superficial venous system. This remarkable ability of the muscle pump is diminished in patients with venous disorders of the lower limbs, resulting in a persistently elevated PEP. In clinical parlance, this is referred to as ambulatory venous hypertension. Side by side, the RT is short from rapid reflux refilling. The pathological situations leading onto development of ambulatory venous hypertension include the following:
Presence of reflux in the saphenous systems
Reflux/obstruction in deep veins
Incompetence of medial calf perforators
In clinical practice, these pathologies exist in combination. But for clarity, they will be considered in isolation.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


