tissue. The somatic component, the pudendal nerve, through the dorsal nerve branches is responsible for penile sensation and the contraction and relaxation of the extracorporeal striated muscles (bulbocavernous and ischiocavernous).
TABLE 24.1 RISK FACTORS ASSOCIATED WITH ED | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
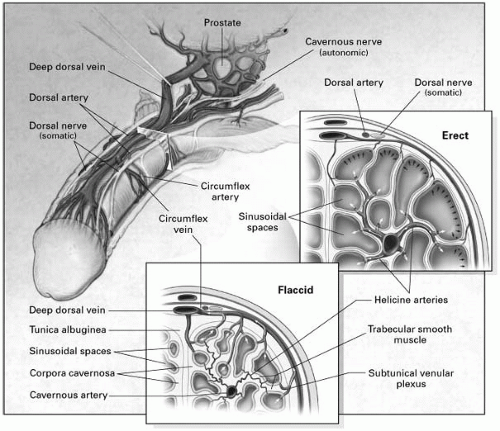 FIGURE 24-1. Anatomy and mechanism of penile erection. The mechanisms of erection and flaccidity are shown in the upper and lower inserts, respectively. During erection, relaxation of the trabecular smooth muscle and dilatation of the arterioles result in an increase in blood flow, which expands the sinusoidal spaces to lengthen and enlarge the penis. The expansion of the sinusoids compresses the subtunical venular plexus against the tunica albuginea and simultaneously compresses the emissary veins, reducing the outflow of blood to a minimum. (From Lue TF. Erectile dysfunction. N Engl J Med 2000;342:1802-1813, with permission.) |
(>20%)]. A careful assessment of subclinical and/or asymptomatic cardiovascular disease should be considered, especially in patients with ED and an estimated cardiovascular risk greater than 10%.
TABLE 24.2 RISK FACTORS ASSOCIATED WITH ED DIFFERENTIAL DIAGNOSIS OF ED | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


