
Fig. 19.1
Menometrorrhagia in a 45-year-old W caused by a poly-myomatous uterus, with a main interstitial-fundic 6-cm myoma. MRI showed that all myomas look uncomplicated. (a) Aortography: injection at the level of L2, showing a normal aortoiliac network and the 2 uterine arteries with symmetric and large diameter, without any large ovarian artery. (b, c) After crossing the aortoiliac bifurcation from a contralateral access, a selective injection was performed in the right hypogastric artery, of which the distribution of the branches was not modal (early phase, 1–2; later phase, 1–3): note that the right uterine artery originates from the first centimeter of the posterior trunk, on its internal edge. (d) Simultaneous injection of both uterine arteries after selective catheterization until their horizontal segment (Cobra hydrophilic 4F catheter): heterogeneous hypervascularization of the uterine fundus, relatively symmetrically provided from the left and right uterine arteries. Note the retro-opacification of the right ovarian artery via the utero-ovarian anastomosis (arrow). (e) End of procedure aortography, showing marked depletion of the arterial vascularization of the uterus
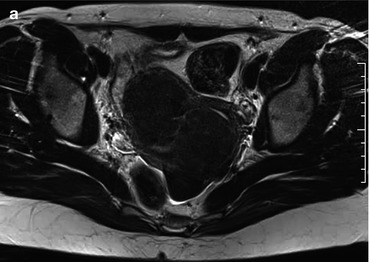
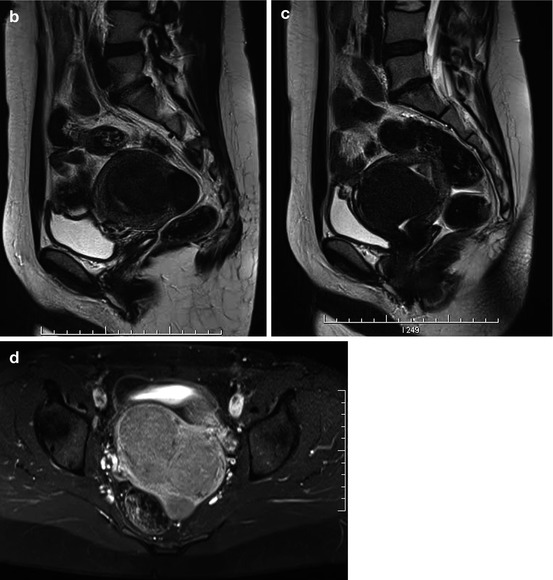
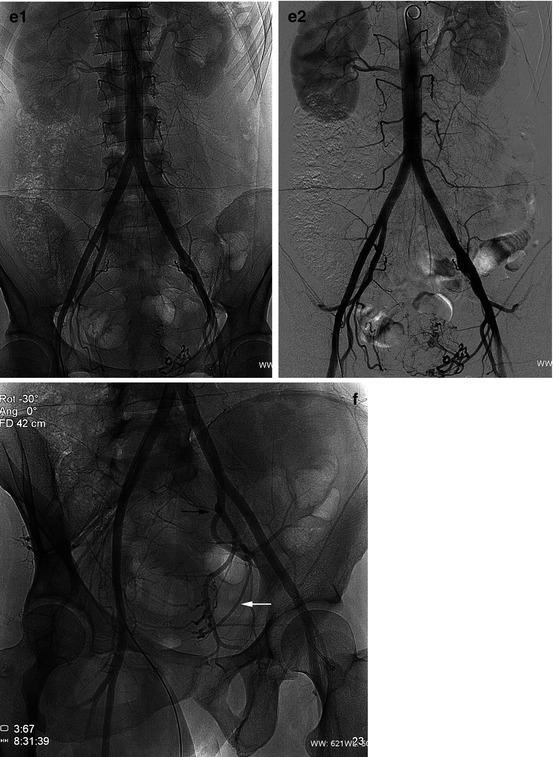
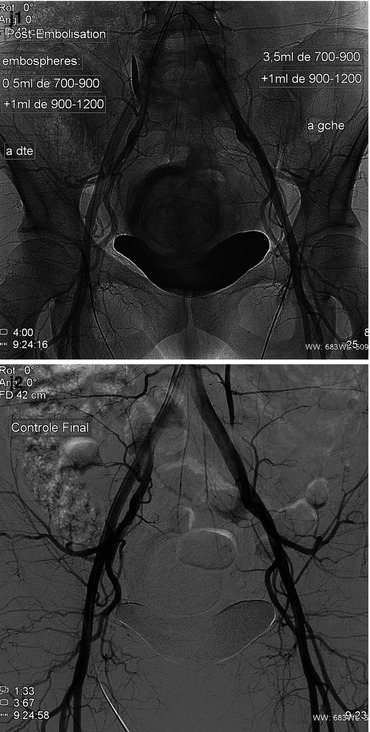

Fig. 19.2
A 40-year-old W, P3, suffering from menometrorrhagia, pollakiuria, constipation, and anemia caused by a myomatous uterus; not any efficacy of progestin treatment. (a–c) Sagittal and transverse T2-weighted MR scans: 3 interstitial low-signal myomas, the largest measuring 5 cm, distorting the contours, and displacing the uterine lumen. (d) T1WI, fat suppression, after gadolinium injection: the three myomas are enhanced. After a multidisciplinary consultation, taking into account the wishes of the patient to preserve her uterus, curative arterial embolization was proposed. (e1, e2) Aortography: normal aortoiliac network; hypervascularization of the uterus. (f) Opacification of the aortoiliac bifurcation (RAO view), showing the hypogastric bifurcation into anterior and posterior trunks (black arrow). It is also possible to identify the uterine artery, originating from the anterior trunk (white arrow). (g1, g2) Hyperselective catheterization of the uterine artery (4 F hydrophilic Cobra catheter), early and late phase: the extremity of the catheter is in the horizontal segment. Uterine hypervascularization, but there is not any specific pedicle nor any utero-ovarian anastomosis. (h) A catheter is in place in the left uterine artery, then tracking the right uterine artery by a crossover from the left femoral artery puncture, followed by an injection at the end of the right hypogastric artery (black arrow) (LAO view): bifurcation into anterior and posterior trunks, very early origin of the uterine artery (white arrow) from the anterior trunk. (i) Selective catheterization of the uterine artery: the right artery seems to be less involved in the vascularization of the uterus (this asymmetric pattern is frequent). Note the mass effect on the bladder. (j1, j2) Aortographic control after embolization: on the right side, 0.5 ml of 700- to 900-μm-diameter microparticles and then 1 ml of 900–1,200-μm particles were injected and, on the left side, 3.5 ml of 700–900 and then 1 ml of 900–1,200 μm. Note the retention of contrast in the myomatous uterus, while only the first few centimeters of the uterine arteries are injected. (k–n) MRI performed 1 year later, while pelvic heaviness disappeared, as well as bleeding and anemia; menorrhagia stays nevertheless described. Compared to pre-embolization MRI: reduction of over 50 % of the diameters of the three fibroids (axial and sagittal T2W, sagittal and axial T1W post gadolinium, fat suppressed); the low T2W signal is unchanged, but the T1W enhancement is significantly reduced



