The aim of the present study was to assess the use of complementary and alternative medicine (CAM) treatments in outpatients with cardiovascular disease and their interest in future use. The increasing popularity of CAM therapies highlights the need to explore their use among patients with cardiovascular disease. Data were collected with a prospective, point-of-care, anonymous, 17-question survey about basic medical information and previous use and interest in the future use of dietary supplements and other CAM interventions among patients undergoing outpatient cardiology evaluation at a Midwestern tertiary care center. The survey was completed by 1,055 patients (655 men, 351 women; mean age 63.5 years) of whom 98.1% were white. Of these, 36.8% had cardiac symptoms for >10 years, 48.2% had coronary artery disease, and 82.5% reported use of CAM therapies. Of these patients, 75.4% reported using dietary supplements, 31.5% chiropractic therapy, 23.9% mind-body therapies, and 19.2% massage. Only 14.4% had discussed the use of CAM treatments with their physicians. The top 4 treatments used for cardiac symptoms were relaxation techniques, stress management, meditation, and guided imagery. Also, 48.6% were interested in participating in a future clinical trial of an alternative treatment. The great majority of patients seen in current practice use CAM therapies, and a large proportion expressed an interest in participating in research with CAM therapies. In conclusion, research directed with an integrative approach to cardiovascular care might prove beneficial when designing future studies.
The definition of complementary and alternative medicine (CAM) has continued to evolve. As defined by the National Center of Complementary and Alternative Medicine, “CAM is a group of diverse medical and healthcare systems, practices, and products that are not generally considered part of conventional medicine.” The 5 categories or domains of CAM as classified by the National Center of Complementary and Alternative Medicine are whole medical systems (e.g., homeopathy, ayurvedic medicine), mind-body interventions (e.g., yoga, tai chi, meditation, qigong, biofeedback, hypnotherapy), biologically based therapies (e.g., herbal treatments, megadose vitamins), manipulative and body-based methods (e.g., chiropractic therapy), and energy therapies (e.g. Reiki, magnetic therapy).
CAM has become increasingly popular in the United States during the past few years. According to a Centers for Disease Control survey in 2007 involving >31,000 patients, almost 40% of adults had used CAM therapies in the previous 12 months. Increasingly, dietary supplements and other CAM treatments are marketed “over the counter” to reduce the risks and symptoms of cardiovascular disease (CVD). In addition, patients with CVD might be more likely to seek CAM treatments to decrease the psychological stress associated with this condition. The proportion of patients with CVD using these treatments has been reported in several studies. However, the data are often reported only for a specific subset of patients (e.g., patients with acute coronary syndrome) or specific interventions (e.g., patients with coronary artery disease practicing mind-body interventions). Furthermore, the proportion of patients with CVD interested in the future use of CAM treatments and the type of interventions preferred by these patients is not yet known. The present study explored, in a point-of-care survey, the proportion of patients with CVD reporting current and/or previous use of CAM treatments. We also evaluated patients’ attitudes toward the future use of CAM treatments.
Methods
The present cross-sectional, point-of-care survey was conducted with patients attending the Cardiology Outpatient Clinic at Mayo Clinic in Rochester, Minnesota, from March 2009 to October 2009. The survey was administered before the clinic consultation. Because the survey did not collect any personal identifiers, no informed consent was obtained. Consent was considered implied by the participant’s completion and return of the survey. The Mayo Clinic institutional review board approved the study protocol.
Patients were included if they were attending an outpatient cardiology appointment; willing and able to participate in the survey; and able to speak, read, and understand the English language. No specific exclusions were used.
A diagnosis of coronary artery disease was implied if 1 of the following 5 questions were checked:
- 1.
Do you suffer from angina pectoris?
- 2.
Have you had an angioplasty?
- 3.
Have you had heart stents placed?
- 4.
Do you have chest pain for which you take nitroglycerin tablets under your tongue?
- 5.
Have you ever had heart bypass surgery?
The study questionnaire was developed in collaboration with the Survey Research Center at the Mayo Clinic. This was a 17-question, paper-and-pencil survey distributed by the desk staff as patients checked in for their cardiology appointment. The participants were given the survey form while waiting for their appointment and were instructed to complete it and return it to the receptionist any time before leaving the clinic.
The anonymous, consecutive survey obtained information on demographic characteristics, CVD history, current CAM use, and attitudes toward the future use of CAM therapies for heart-related symptoms. CAM use was stratified into dietary supplements and other CAM modalities. The survey instrument required approximately 15 to 20 minutes to complete. The response categories varied, depending on the specific question asked.
The data were summarized using frequency distribution tables stratified by gender for all categorical variables. The Fisher exact test or chi-square test was used to compare the categorical data between the 2 groups. p Values <0.05 were considered statistically significant.
Results
Of the 1,055 patients surveyed, 655 (65%) were men and 351 (35%) were women ( Table 1 ). No difference was seen in age of the men and women who completed the survey. Virtually all the participants (98.1%) were white. Of those surveyed, 367 (36.8%) had heart-related symptoms for >10 years, with 163 (16.2%) reporting current symptoms of angina pectoris requiring the use of sublingual nitroglycerin. A diagnosis of coronary artery disease was reported by 507 participants (48.2%), and 43 patients (4.3%) were current smokers. Of those surveyed, 57.4% of patients had coexisting hypertension, 51.6% had hyperlipidemia, and 28.5% had a diagnosis of gastroesophageal reflux disease. The duration of cardiac symptoms and a history of coronary artery disease, myocardial infarction, angiography, or revascularization were greater for the men.
| Characteristic | Overall (n = 1,055) | Men (n = 655) | Women (n = 351) ∗ | p Value † |
|---|---|---|---|---|
| Age (yrs) | 0.09 | |||
| Mean ± SD | 63.5 ± 14.52 | 64.1 ± 14.25 | 62.4 ± 14.92 | |
| Range | 5.0–99.0 | 5.0–99.0 | 10.0–99.0 | |
| Race | 0.35 | |||
| White | 972 (98.1%) | 632 (98.3%) | 337 (97.7%) | |
| Black | 3 (0.3%) | 3 (0.5%) | 0 | |
| American Indian/Alaskan native | 9 (0.9%) | 5 (0.8%) | 4 (1.2%) | |
| Asian | 6 (0.6%) | 3 (0.5%) | 3 (0.9%) | |
| Native Hawaiian/other Pacific Islander | 1 (0.1%) | 0 | 1 (0.3%) | |
| Heart-related symptom duration (yrs) | 0.02 | |||
| <1 | 175 (17.6%) | 118 (18.8%) | 51 (15.7%) | |
| 1–3 | 185 (18.6%) | 105 (16.7%) | 68 (20.9%) | |
| 4–5 | 105 (10.5%) | 58 (9.2%) | 41 (12.6%) | |
| 6–10 | 165 (16.5%) | 97 (15.4%) | 62 (19.1%) | |
| >10 | 367 (36.8%) | 251 (39.9%) | 103 (31.7%) | |
| Angina pectoris | 163 (16.2%) | 94 (14.8%) | 63 (19.2%) | 0.02 |
| Sublingual nitroglycerin tablet use | 164 (16.2%) | 105 (16.7%) | 55 (16.3%) | 0.98 |
| Previous coronary angiography | 465 (46.4%) | 312 (49.4%) | 129 (39.1%) | 0.006 |
| Angioplasty or heart stents placed | 271 (58.3%) | 198 (63.5%) | 60 (46.5%) | 0.001 |
| Previous heart bypass surgery | 197 (20.2%) | 154 (24.9%) | 34 (10.8%) | <0.001 |
| Coronary artery disease | 507 (48.2%) | 341 (52.1%) | 139 (39.8%) | <0.001 |
| Currently smoke cigarettes | 43 (4.3%) | 27 (4.1%) | 16 (4.6%) | 0.74 |
| Discussed use of alternative treatments with physician | 135 (14.4%) | 78 (12.7%) | 57 (17.6%) | 0.04 |
| Interested in participating in clinical trial | 471 (48.6%) | 302 (47.3%) | 166 (50.9%) | 0.28 |
| Diagnosed medical conditions (most to least common overall) | ||||
| High blood pressure | 606 (57.4%) | 374 (57.1%) | 199 (56.7%) | 0.90 |
| High cholesterol | 544 (51.6%) | 343 (52.4%) | 173 (49.3%) | 0.35 |
| Acid reflux | 301 (28.5%) | 176 (26.9%) | 114 (32.5%) | 0.06 |
| Heart attack | 241 (22.8%) | 174 (26.6%) | 53 (15.1%) | <0.001 |
| Diabetes | 187 (17.7%) | 120 (18.3%) | 59 (16.8%) | 0.55 |
| Heart failure | 175 (16.6%) | 116 (17.7%) | 53 (15.1%) | 0.29 |
| Angina pectoris | 166 (15.7%) | 114 (17.4%) | 47 (13.4%) | 0.10 |
| Stroke | 95 (9.0%) | 61 (9.3%) | 33 (9.4%) | 0.96 |
| Lung disease | 92 (8.7%) | 58 (8.9%) | 33 (9.4%) | 0.77 |
| Coronary spasm | 45 (4.3%) | 25 (3.8%) | 19 (5.4%) | 0.24 |
| Total diagnosed conditions (n) | ||||
| Median (IQR) | 2 (1–3) | 2 (1–3) | 2 (1–3) | |
| Range | 0–9 | 0–9 | 0–8 |
∗ Data not provided by 49 participants for gender.
Overall, 863 patients (81.8%) reported previous use of CAM therapies. Of these, 466 participants (44.2%) reported the use of CAM therapies for heart-related symptoms. The use of dietary supplements was reported by 795 participants (75.4%), and the use of CAM approaches other than dietary supplements was reported by 550 (52.1%). Of those surveyed, 252 (23.9%) reported using mind-body therapy.
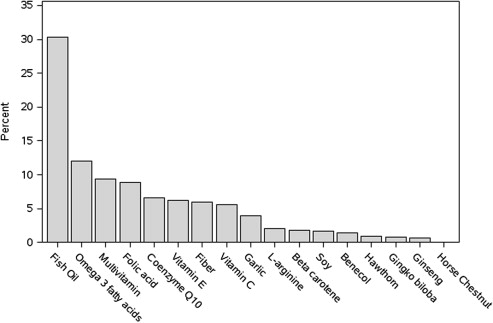
The top 5 dietary supplements used were multivitamins (52.8%), fish oil (45.2%), vitamin C (36.1%), vitamin E (29.0%), and fiber (27.1%; Table 2 ). The top supplements used for heart-related conditions were fish oils, omega 3 fatty acids, multivitamins, folic acid, coenzyme Q10, and vitamin E ( Figure 1 ).
| Dietary Supplement | Any Use (n = 1,055) | Previously for Heart Symptoms (n = 1,055) | Currently for Heart Symptoms (n = 1,055) |
|---|---|---|---|
| Multivitamin | 557 (52.8%) | 54 (5.1%) | 64 (6.1%) |
| Fish oil | 477 (45.2%) | 158 (15.0%) | 213 (20.2%) |
| Vitamin C | 381 (36.1%) | 40 (3.8%) | 28 (2.7%) |
| Vitamin E | 306 (29.0%) | 53 (5.0%) | 19 (1.8%) |
| Fiber | 286 (27.1%) | 32 (3.0%) | 43 (4.1%) |
| Omega 3 fatty acids | 244 (23.1%) | 81 (7.7%) | 72 (6.8%) |
| Folic acid | 193 (18.3%) | 63 (6.0%) | 47 (4.5%) |
| Coenzyme Q10 | 125 (11.8%) | 42 (4.0%) | 40 (3.8%) |
| Garlic | 123 (11.7%) | 31 (2.9%) | 14 (1.3%) |
| Soy | 73 (6.9%) | 13 (1.2%) | 7 (0.7%) |
| Gingko biloba | 57 (5.4%) | 7 (0.7%) | 2 (0.2%) |
| β Carotene | 52 (4.9%) | 16 (1.5%) | 7 (0.7%) |
| l -Arginine | 40 (3.8%) | 15 (1.4%) | 7 (0.7%) |
| Ginseng | 39 (3.7%) | 6 (0.6%) | 2 (0.2%) |
| Benecol | 27 (2.6%) | 11 (1.0%) | 7 (0.7%) |
| Hawthorn | 13 (1.2%) | 8 (0.8%) | 2 (0.2%) |
| Horse chestnut | 4 (0.4%) | 1 (0.1%) | 0 |
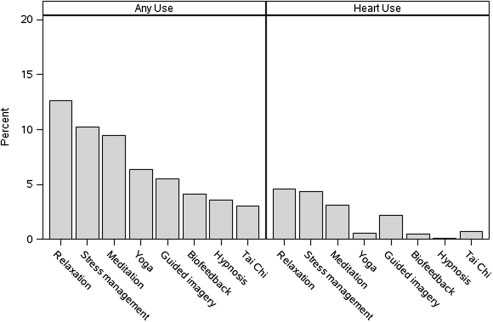
The top 4 CAM modalities other than dietary supplements were chiropractic therapy (31.5%), massage (19.2%), relaxation techniques (12.6%), and stress management techniques (10.2%; Table 3 ). For heart-related symptoms, the top 4 CAM treatments used were relaxation programs (4.5%), stress management (4.4%), meditation (3.1%), and guided imagery (2.2%). Among patients using mind-body therapies, the most popular approaches used were relaxation techniques (12.6%), stress management (10.2%), and meditation (9.5%; Figure 2 ).
| Treatment | Any Use (n = 1,055) | Previously for Heart Symptoms (n = 1,055) | Currently for Heart Symptoms (n = 1,055) |
|---|---|---|---|
| Chiropractic therapy | 332 (31.5%) | 10 (0.9%) | 3 (0.3%) |
| Massage | 203 (19.2%) | 4 (0.4%) | 5 (0.5%) |
| Relaxation | 133 (12.6%) | 34 (3.2%) | 29 (2.7%) |
| Stress management | 108 (10.2%) | 31 (2.9%) | 28 (2.7%) |
| Meditation | 100 (9.5%) | 28 (2.7%) | 20 (1.9%) |
| Acupuncture | 96 (9.1%) | 6 (0.6%) | 5 (0.5%) |
| Yoga | 67 (6.4%) | 4 (0.4%) | 4 (0.4%) |
| Guided imagery | 58 (5.5%) | 19 (1.8%) | 5 (0.5%) |
| Biofeedback | 43 (4.1%) | 3 (0.3%) | 2 (0.2%) |
| Hypnosis | 38 (3.6%) | 1 (0.1%) | 0 |
| Acupressure | 32 (3.0%) | 4 (0.4%) | 3 (0.3%) |
| Reflexology | 32 (3.0%) | 2 (0.2%) | 2 (0.2%) |
| Tai chi | 32 (3.0%) | 5 (0.5%) | 5 (0.5%) |
| Homeopathy | 28 (2.7%) | 5 (0.5%) | 2 (0.2%) |
| Magnetic therapy | 21 (2.0%) | 3 (0.3%) | 0 |
| Naturopathy | 8 (0.8%) | 1 (0.1%) | 0 |
| Ayurvedic treatment | 7 (0.7%) | 1 (0.1%) | 2 (0.2%) |
The most common heart-related symptoms for which patients reported using CAM treatments were shortness of breath, palpitations, chest pain, dizziness, and leg swelling. Of the patients using CAM therapy for heart-related symptoms, the greatest benefit was reported for palpitations (22.2%), sleep disturbance (21.8%), chest pain (20.0%), and leg swelling (19.4%; Table 4 ). Among patients with coronary artery disease, the greatest benefit was reported for chest pain (20.0%), sleep disturbance (17.9%), leg swelling (17.9%), and shortness of breath (13.9%). Among those without coronary artery disease, the greatest benefit was reported for palpitations (32.8%), sleep disturbance (26.3%), leg swelling (25.0%), and shortness of breath (24.1%).



