Congenitally corrected transposition of the great arteries (l-TGV, l-TGA)
As mentioned earlier, the term transposition means a reversal of anteroposterior anatomic relationships. Therefore, in transposition of the great arteries, the aorta arises anteriorly and the pulmonary artery arises posteriorly. Normally, the anterior blood vessel arises from the infundibulum, which is the outflow portion of the morphologic right ventricle.
In congenitally corrected transposition of the great arteries, these anatomic relationships are present and the circulation is physiologically correct (i.e. systemic venous return is delivered to the pulmonary arteries; pulmonary venous return is delivered to the aorta).
The anatomy of congenitally corrected transposition of the great arteries differs from complete transposition of the great arteries (d-TGV) because ventricular inversion coexists. The term inversion indicates an anatomic change in the left–right relationships. Therefore, inversion of the ventricles indicates that the morphologic right ventricle lies on the left side and that the morphologic left ventricle lies on the right side. The inversion of the ventricles in corrected transposition of the great arteries allows the circulation to flow in a normal pattern (Figure 7.1).
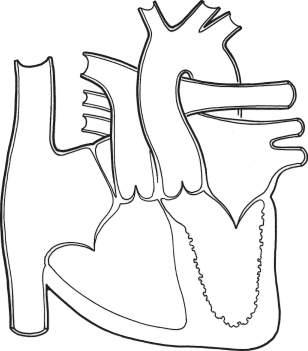
Figure 7.1 Congenitally corrected transposition of the great vessels (l-TGV, l-TGA). In addition to levo-transposed great vessels, ventricular inversion is found. The morphologic right ventricle (trabeculated) is left-sided and is located between the left atrium (fully oxygenated blood) and the aorta. The morphologic left ventricle is right-sided and is positioned between the right atrium (deoxygenated blood) and the pulmonary artery. Therefore, the circulation is physiologically correct.
The systemic venous return from the inferior and superior venae cavae passes into the normally positioned right atrium. This blood then flows across a mitral valve into a ventricle that has these morphologic features of a left ventricle: it is a finely trabeculated chamber, and fibrous continuity exists between the atrioventricular (mitral) and semilunar valves (pulmonary). This ventricle is located to the right of the other ventricle. This anatomic left ventricle ejects blood into a posteriorly and medially placed pulmonary artery.
The pulmonary venous blood returns into the normally placed left atrium. The flow then crosses a tricuspid valve into a ventricle having the morphologic features of a right ventricle: it is coarsely trabeculated and the atrioventricular (tricuspid) and semilunar valves (aortic) are separated by an infundibulum. The aorta arises from the infundibulum and lies anteriorly and left of the pulmonary artery.
The flow of blood, therefore, is normal and the anatomic relationship of the great vessels fulfills the definition of transposition of the great arteries. This type of transposition has also been termed levo-transposition because the aorta lies to the left of the pulmonary artery.
This condition alone would lead to no cardiovascular symptoms or murmurs (although there are concerns of the ability of the systemic ventricle to sustain the systemic circulation). Virtually all patients with congenitally corrected transposition, however, have coexisting cardiac anomalies. Ventricular septal defect, pulmonary stenosis, and insufficiency of the left-sided atrioventricular valve are the most common associated cardiac anomalies.
These coexistent anomalies lead to clinical and laboratory findings similar to those found in patients with the same anomaly but with normal relationships between the ventricles and the great vessels.
Three clinical findings, however, allow the detection of congenitally corrected transposition of the great arteries as the underlying cardiac malformation:
Patients with congenitally corrected transposition of the great arteries often spontaneously develop partial or complete heart block.
While the basic anatomic anomaly in congenitally corrected transposition of the great arteries does not require treatment, hemodynamically significant coexistent conditions do, generally by operation.
Operative treatment
The associated anomalies are corrective using the same general techniques as in those with normally related ventricles and great arteries. The treatment of the Ebstein’s anomaly is challenging because the basic approach to the operation on the valvar condition varies. Additionally, as in any patient with left AV valve regurgitation, it is critical that the operation reduces the degree of regurgitation. Because of the concern about the ability of the inverted right ventricle to function adequately for a long period at systemic levels of pressure, this has prompted selected centers to perform a “double switch” procedure. This involves performing an arterial switch so that the aorta is connected to the left ventricle and the pulmonary artery is connected to the right ventricle. This creates the circulatory pattern of complete transposition. To address this, an atrial switch is carried out during the same operation so that systemic venous blood flows to the right ventricle and then to pulmonary artery. Pulmonary venous blood is directed to the left ventricle and then aorta. This approach is in a developmental stage, so its broad use is limited.
Natural history
The natural history is affected by three issues. The first determinate is the nature and severity of the coexistent cardiac condition. If the condition is significant, it will require correction or palliation early in life. Second, there is a 2% annual development of heart block which requires treatment. Finally, systemic right ventricular dysfunction develops often by the third decade and requires anticongestive measures.
Malposition of the heart
The heart may assume an abnormal position in either the left or the right side of the chest. Various classifications of cardiac malposition have been developed, but the authors favor the one presented here, although the terminology may differ from that of other authors.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


