Fig. 12.1
Ultrasound-guided puncture: Right axillary arterial access with ultrasound-guided puncture for ductal stenting of a complex ductus-dependent defect in a 3-day-old infant with a BW of 2.9 kg. A 4.5–11.5 MHz ultrasound probe (GE Healthcare, Wauwatosa, USA) was used to visualize the axillary artery, and percutaneous puncture was performed with a 20G Abbocath. After vessel puncture and wire placement, a 3 French sheath (Balt, Montmorency, France) was introduced percutaneously and stent implantation (Coroflex blue) was performed
Ultrasound-guided puncture may also be used for uncommon vascular approaches such as transhepatic access.
12.3 Transhepatic Vascular Access
In patients with caval thrombosis or vascular malformation (absent SVC, IVC, or azygos continuation), those central vessels (caval veins or atrium) may not be accessible via conventional approaches. If the femoral or jugular access routes are obstructed or missing, a transhepatic approach may allow diagnostic or therapeutic catheterization or placement of a central venous line [2]. Transhepatic puncture is performed using the ultrasound-guided approach after sonographic visualization of the liver structure and especially liver veins [1]. We perform percutaneous puncture from the lateral or medial position after visualization of the concomitant structures and vessels. After passing the liver parenchyma, the liver veins should be reachable with the proximal part of the needle and aspiration should be attempted. If a withdrawal of blood is possible, correct position may be checked again by ultrasound and the introduction wire may be advanced into the atrium of the heart. Thereafter, the sheath or central catheter may be placed with or without pre-dilatation. The presence of hematoma can be excluded sonographically and liver enzymes checked, if a central line remains in place (Fig. 12.2).
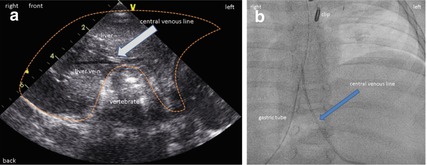
Fig. 12.2
Transhepatic central venous line placement: ultrasound-guided puncture by a left paravertebral and median percutaneous approach due to inverse abdominal situs with dextrocardia in a patient with caval thrombosis. (a) Sonographic picture after transhepatic placement of the central venous line. Visualization of liver veins and liver tissue is essential for percutaneous approach. (b) Fluoroscopic picture of central venous line with a transhepatic approach
12.4 Paravertebral Access
The vertebral–azygous–hemiazygous pathway may exhibit significantly enlarged collateral vessels in patients after corrective surgery of congenital heart disease, especially in those with modified Glenn or TCPC/Fontan operations or with obstructions or thrombosis of the superior caval vein. In these patients, the collateral pathways may connect to the pulmonary veins via the bronchial vascular system, potentially giving rise to a significant right-to-left shunt and, in some cases, cyanosis. With connection to the paravertebral veins, the vessels are often located extremely posterior, making retrograde access from the systemic or pulmonary veins difficult or impossible. In some cases, the proximal region may already have been occluded, but collateral flow still exists. MRI or computed tomographic visualization of the azygous or hemiazygous veins and their collateral vessels with CT-guided access through the paravertebral veins makes it technically possible to reach the vessel and applies a transcatheter occlusive strategy (see Fig. 12.4). Despite the direct proximity to the pleura, access to the paravertebral veins may only be possible with a high degree of precision under real-time CT-based navigation. Thus, this approach can be recommended whenever access to the paravertebral veins is deemed mandatory.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


