Fig. 1
Chest X-ray showing a left-sided pleural effusion and an elevated left hemidiaphragm
A thoracic CT scan revealed a large amount of free pleural fluid (50 HU), which constricts lung parenchyma and causes its atelectasis. Moreover, the presence of a tumor in the left hilum, measuring 77 × 48 mm, was suspected (Fig. 2).
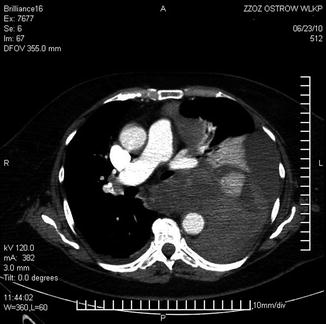
Fig. 2
Contrast enhanced CT scan showing fluid accumulation which constricts lung parenchyma and the suspicion of a tumor in the left hilum, measuring 77 × 48 mm in cross section
A suction chest drain was inserted because of the hemothorax. Over 1,000 ml of blood was removed. The patient was then transferred to the regional pulmonary center. A bronchoscopy was performed and no pathology in the bronchial tree was discovered. A chest ultrasound revealed a 59 mm thick layer of fluid in the left hemithorax. A thoracotomy was recommended in order to perform a hematoma debridement and a decortication with a subsequent tissue biopsy. Therefore, the patient was admitted to the department of thoracic surgery in July 2010 (No 33270/2010). The patient was hemodynamically stable (BP 110/90 mmHg). Blood tests revealed a hemoglobin level of 8.4 g/dl. The patient received two units of packed red blood cells (pRBC). Informed consent was obtained. The patient was administered a general anesthesia with a double lumen endotracheal intubation. A left anterolateral thoracotomy approach was used. Approximately 2,000 ml of semi-clotted blood was aspirated. As there were dense intrapleural adhesions, a decortication was performed. The mediastinal pleura below the aortic arch was incised and it seemed to the surgeon that there was an organized blood clot which was 6 cm in diameter. When the “clot” was removed from the mediastinum, active arterial bleeding started. The source of the hematoma was in this way identified and ligated. Two thoracostomy tubes were inserted. Routine monitoring of vital signs was performed postoperatively. A second-generation cephalosporin was administered for 24 h. The postoperative course was uncomplicated. The patient was discharged on the 7th postoperative day. Surprisingly, the final pathology examination of the formalin-fixed paraffin-embedded (FFPE) tissue revealed malignant spindle cell neoplasm, probably a sarcoma (Fig. 3).
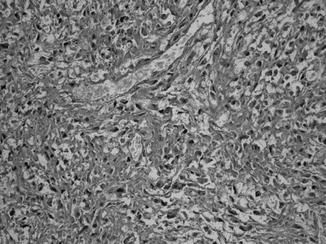




Fig. 3
Malignant spindle cell neoplasm, probably a sarcoma. There are necrotic masses and spindle-shaped cells with nuclear polymorphism, atypia, and nets of reticular fibers (hematoxylin and eosin stain, magnification 200×)
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
