Tumors and Other Mass Lesions
Although cardiac tumors can often be seen on transthoracic echocardiography (TTE), their location, size, and relation to surrounding structures are better defined by transesophageal echocardiography (TEE).
The most common primary cardiac tumor is the myxoma. This tumor rarely metastasizes, but it can cause obstruction and frequently embolize, making its immediate removal mandatory. These tumors can also cause regurgitation by interfering with valve function, and they can cause a variety of constitutional symptoms. Myxomas are usually solitary and are located most commonly in the left atrium. However, because they can occur in any chamber and may be multiple, a careful transesophageal echocardiographic investigation of all the cardiac chambers should be conducted preoperatively to be certain that all tumors have been detected and are removed. Myxomas characteristically have cystic spaces caused by hemorrhages and areas of calcification. The base of the tumor may be either broad or narrow, and a careful search should be made for the attachment point. In one patient we studied there was massive calcification that involved the left atrial free wall and protruded into the left atrial cavity, mimicking a myxoma. Heavy mitral annular calcification may also produce a confusing picture, especially if some areas are soft and mobile. Lipomas are characteristically more refractile than a noncalcified myxoma, which may help in distinguishing between them. Tumors such as a leiomyoma or leiomyosarcoma may arise from the wall of a blood vessel and cause obstruction to blood flow. Fibroelastomas often present as irregular mobile masses on valves or chamber walls, emanating from narrow stalks. Because of their embolic potential they should be surgically removed. Large mobile vegetations attached to valves may mimic fibroelastoma or a small myxoma on a valve, but the associated clinical picture, which is suggestive of infective endocarditis, helps in differentiating between them. They must be distinguished from Lambl’s excrescences, which are a normal finding in many adults. These are filamentous mobile avascular structures that generally arise at the line of closure of valves and are common in adults. Fibroelastomas are not as thin as Lambl’s excrescences and, unlike Lambl’s excrescences, they do not arise from the line of closure, but from elsewhere on the valve. Myxomatous thickening or nodules involving the mitral valve may also simulate a small tumor.
Thrombus can mimic a tumor, and the distinction often cannot be made by echocardiography. As with tumors, identifying the point of attachment is important in surgical planning. Although low-flow velocities are often present (and are, indeed, causative) when a thrombus is found, this may not always be the case, and thrombi can occur in the absence of an identifiable precipitating factor. TEE is more sensitive than TTE for the detection of thrombi, particularly in the atrial appendages. Thrombi are generally broad based, rather than pedunculated, and are hyperechoic relative to the myocardium except that there tends to be an echolucent interface between the thrombus and the atrium. This echolucent interface may be used to try to differentiate the thrombus from the tumor, but from a practical point of view, echocardiographic differentiation of the tumor from the thrombus is frequently not feasible.
Thrombi originating in the heart are most often, but not invariably, associated with low-flow regions. In the left ventricle, thrombi commonly attach to hypokinetic or akinetic wall regions, ventricular aneurysms, or occur in the setting of cardiomyopathy.
In the left atrium, thrombus can occur anywhere, but most commonly arises in the left atrial appendage, which is far better imaged with TEE than with TTE. On TEE, the left atrial appendage thrombus must be differentiated from the pectinate muscles and from septa between multiple lobes that not infrequently make up the left atrial appendage. Spontaneous contrast, which occurs characteristically with slow flow, is caused by red blood cell aggregation and is a risk factor for the development of thrombus.
When thrombi originate in the right atrium, indwelling catheters or pacemaker leads are frequently
the cause, although migrating emboli from lower extremity veins are occasionally visualized. Interestingly, during transesophageal examination we have visualized thrombi, subsequently confirmed by both surgery and pathology, attached to the mitral valve and in the region of papillary muscles in the normally functioning left and right ventricles, with no clinically or echocardiographically discernible cause. Right-sided tumors must be differentiated from normal structures such as hypertrophied trabeculations in the right atrium or right ventricle and prominent or hypertrophied right ventricular papillary muscles. A prominent eustachian or thebesian valve and Chiari network, as well as a prominent crista terminalis visualized at the junction of the superior vena cava and the right atrium, may also be mistaken for a tumor mass. Abnormal thickening of normal structures, such as lipomatous hypertrophy of the interatrial septum or nonspecific thickening of the “Q-tip” (i.e., left atrial wall invagination or infolding separating the appendage from the left upper pulmonary vein) also may mimic tumor infiltration.
the cause, although migrating emboli from lower extremity veins are occasionally visualized. Interestingly, during transesophageal examination we have visualized thrombi, subsequently confirmed by both surgery and pathology, attached to the mitral valve and in the region of papillary muscles in the normally functioning left and right ventricles, with no clinically or echocardiographically discernible cause. Right-sided tumors must be differentiated from normal structures such as hypertrophied trabeculations in the right atrium or right ventricle and prominent or hypertrophied right ventricular papillary muscles. A prominent eustachian or thebesian valve and Chiari network, as well as a prominent crista terminalis visualized at the junction of the superior vena cava and the right atrium, may also be mistaken for a tumor mass. Abnormal thickening of normal structures, such as lipomatous hypertrophy of the interatrial septum or nonspecific thickening of the “Q-tip” (i.e., left atrial wall invagination or infolding separating the appendage from the left upper pulmonary vein) also may mimic tumor infiltration.
Malignant tumors of the heart are unusual but, when present, they tend to metastasize early. They can often be recognized on the basis of the fact that they deform the walls of the heart. Other tumors, such as melanoma, may produce blood-borne metastases in the heart. Mediastinal tumors such as a leiomyosarcoma may compress or invade the heart, either directly or through vascular accesses such as the pulmonary veins. Because these tumors are vascular, multiple small blood vessels may be imaged within the tumor by color Doppler, especially if the Nyquist limit is kept low. Sclerosing mediastinitis producing narrowing of the systemic and pulmonary veins at their junction with the heart may simulate an extracardiac tumor. Postoperative hematomas also must be differentiated from extracardiac tumor masses.
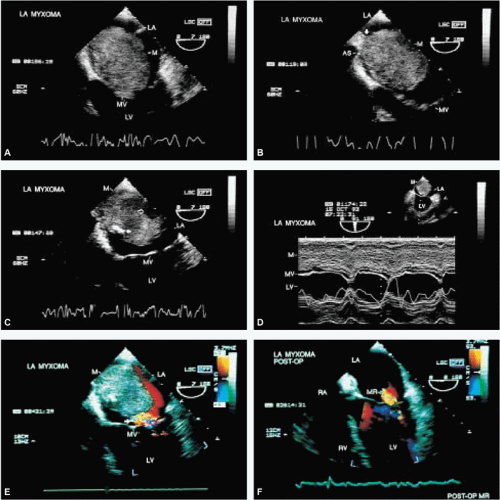 FIGURE 9.1. Left atrial myxoma. A–F. A huge left atrial (LA) myxoma (M) with a broad attachment on the atrial septum (AS, arrow in B). C. An area of calcification (closed arrow) in the tumor and an echolucency caused by hemorrhage (open arrow). D. M-mode study of the tumor. E. Associated mild mitral regurgitation (MR) (arrow). F. Postoperative study after removal of the myxoma shows persistence of mild MR. LA, left atrium; LV, left ventricle; MV, mitral valve; RA, right atrium; RV, right ventricle. |
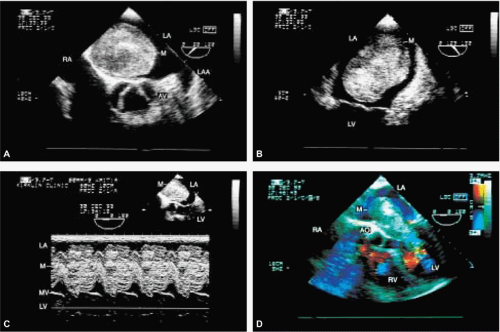 FIGURE 9.2. Left atrial myxoma. A–D. A huge myxoma (M) is seen in the left atrium (LA) obstructing the mitral orifice in diastole (D). AO, aorta; AV, aortic valve; LAA, left atrial appendage; LV, left ventricle; MV, mitral valve; RA, right atrium. |
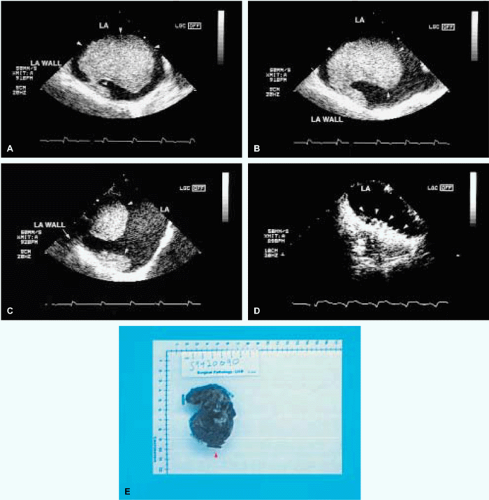 FIGURE 9.4. Left atrial tumor mimic. A,B. A huge nonmobile mass (arrowheads) consistent with a tumor in the left atrium (LA). It appeared to have a broad attachment to the LA free wall (B). C. Spontaneous contrast echoes in LA next to the mass, which was successfully removed. D. The suture line (arrowheads) repairing the LA wall following its resection. E. The resected mass, which was found to be a thrombus and not a tumor at pathology. No etiologic factors were identified. |
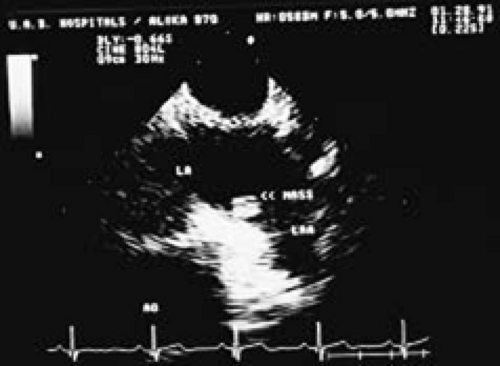 FIGURE 9.5. Left atrial tumor. A small mass consistent with a tumor is seen at the base of the left atrium (LA) appendage in this patient, who presented with symptoms of an embolic stroke. AO, aorta; LAA, left atrial appendage. |
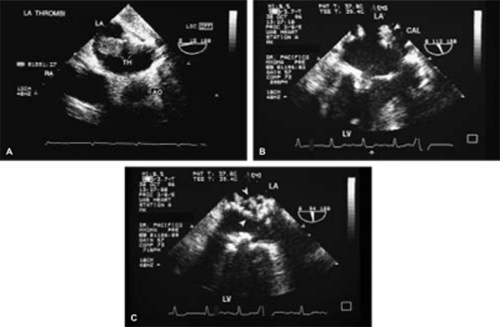 FIGURE 9.6. Left atrial thrombus/calcification. A. Two large thrombi (TH) are seen in the left atrium (LA). These could be distinguished from tumor by their mobility and the presence of spontaneous contrast echoes seen in other views. B,C. In another patient, heavy calcifications (CAL, arrows) involving the LA free wall are seen protruding into the LA cavity and mimicking a tumor. The findings were verified at surgery and by pathologic examination. AO, aorta; LV, left ventricle; RA, right atrium. |
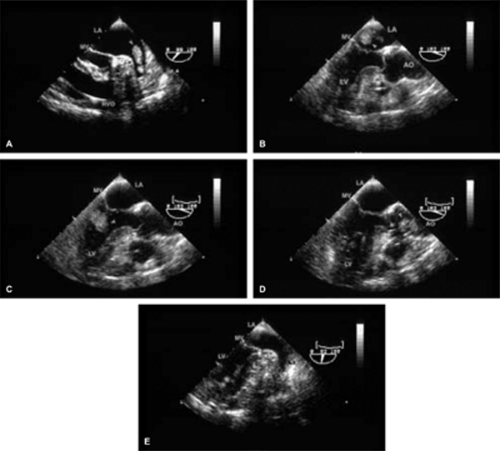 FIGURE 9.7. Sequential echocardiographic images showing dislodgement of the left atrial appendage (LAA) thrombus (TH) (arrowhead in A) and its subsequent journey into the left atrium (LA) (B) through the mitral valve (MV) into the left ventricle (LV) (C), and then into the ascending aorta (AA) (D). No residual TH is seen in the LAA (arrowhead in E) subsequent to the peripheral embolization. AO, ascending aorta; LV, left ventricle; RVO, right ventricular outflow tract. (Reproduced with permission from Nekkanti R, Nanda, NC. Left atrial appendage thrombus in transit with peripheral embolization. Am J Geriatr Cardiol 2002;11:60–61. ) |
 FIGURE 9.8. Left atrial tumor mimic. A,B. Nonspecific thickening (arrows) of the invaginated/infolded part of the left atrium (LA) free wall “Q-tip” mimicking a tumor. LA wall infolding is a normal finding at the site where the left upper pulmonary vein (LUPV) enters into the LA and appears as a “septum” separating the LUPV from the left atrial appendage (LAA). AV, aortic valve; RVO, right ventricular outflow tract. |
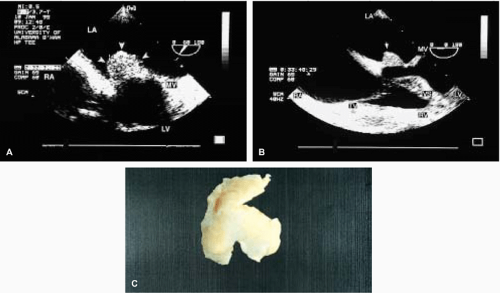 FIGURE 9.9. Mitral valve myxoma. A,B. A large tumor (arrows) attached to the atrial aspect of the anterior mitral leaflet. The multiple tiny echolucencies seen within the tumor suggest the presence of hemorrhage, often seen in myxomas. C. The resected specimen. LA, left atrium; LV, left ventricle; Mitral valve (MV) RA, right atrium; RV, right ventricle; TV, tricuspid valve; VS, ventricular septum. |
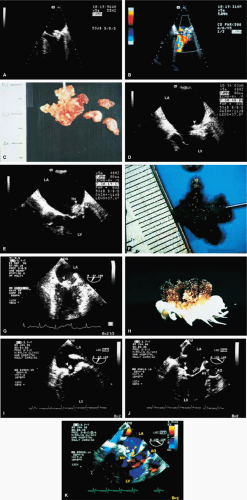 FIGURE 9.10. Mitral valve thrombus/myxomatous degeneration. A–C. The prominent echodensity involving the posterior mitral leaflet (PML) was identified as a thrombus (TH) at surgery and on pathologic examination. B. Mild mitral regurgitation (MR) is noted. The arrowheads in (D,E, and G) show two other patients with masses involving the mitral valve (MV) that were found to be thrombi at surgery and pathology. F,H. The resected thrombi from these two patients. No predisposing factors were identified in any of the three patients shown here. I–K. A different patient with a small rounded mass (arrowheads) attached to the base of the PML. The MV showed prolapse and mild MR (arrow in K). Pathologic examination of the resected mass showed myxomatous degenerative changes and no evidence of tumor. AML, anterior mitral leaflet. |
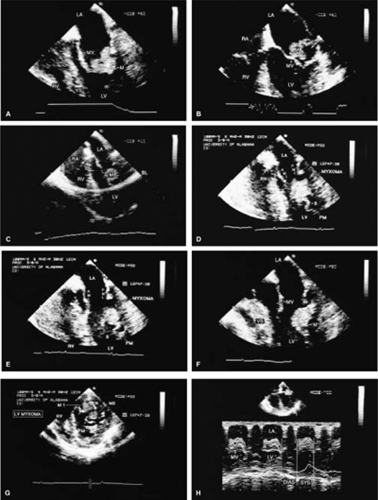 FIGURE 9.11. Left ventricular myxoma. A–C. A large mass (M) in the left atrium (LA) that appears to be attached to the anterior mitral leaflet (AML). D–F. Further examination showed that the mass actually arose from the left ventricle (LV) and was attached by a long stalk (S) to a papillary muscle (PM). G. In the short-axis view, two separate masses (M1 and M2) together with two separate stalks (arrows) were identified in the region of the papillary muscles. H. An M-mode study demonstrates the mass in the LA only during systole. Note a large arc-like side-lobe (SL) artifact in C. Because of the long stalk, one of the myxomas intermittently prolapsed into the LA, sometimes becoming trapped in that chamber. These tumors were successfully resected. PML, posterior mitral leaflet. (A and G reproduced with permission from Samdarshi TE, Mahan EF III, Nanda NC, et al. Transesophageal echocardiographic diagnosis of multicentric LV myxomas mimicking a left atrial tumor. J Thorac Cardiovasc Surg 1992;103:471–474. ) LA, left atrium; LV, left ventricle; M, myxoma; M1 and M2, two separate masses; MV, mitral valve; RA, right atrium; RV, right ventricle; VS, ventricular septum. |
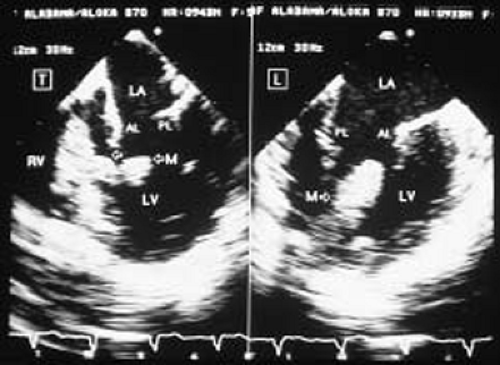 FIGURE 9.12. Left ventricular myxoma. A large mass (M; arrows) arising from the apex. Pathology examination demonstrated it to be a myxoma. AL, anterior mitral leaflet; PL, posterior mitral leaflet. LA, left atrium; LV, left ventricle; M, myxoma; RV, right ventricle; T, transverse plane. (Reproduced with permission from Nanda NC, Pinheiro L, Sanyal RS, et al. Transesophageal biplane echocardiographic imaging: technique, planes, and clinical usefulness. Echocardiography 1990;7:771–788. ) |
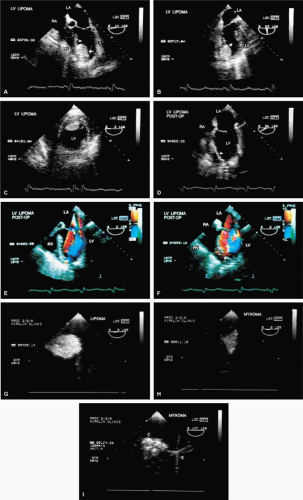 FIGURE 9.13. Left ventricular lipoma. A. The lower arrow shows a bright, highly echogenic, and generally homogeneous mass arising from the apical portion of the ventricular septum. The mass (arrow, T) was also well seen in the two-chamber (B) and short-axis (C) views. This elderly female patient underwent angioplasty of the proximal left anterior descending coronary artery subsequent to an episode of chest pain, and the mass was discovered on a follow-up two-dimensional echocardiogram. Consequently, thrombus was considered in the differential diagnosis, along with myxoma and lipoma. There were no obvious wall motion abnormalities. The mass was surgically removed and found to be a lipoma. D. Patch repair (arrow) of the apical ventricular septum following lipoma resection. E,F. Mild turbulence (arrows) is seen in the region of the patch, but no defect is present. The resected lipoma and a myxoma removed from another patient were studied in vitro by suspending them in a water bath using the same transesophageal probe used for the in vivo study. At the same instrument settings and similar distance from the transducer surface, the lipoma (G) appeared to be significantly hyper-refractile compared to the myxoma (H), except for the areas of calcifications (C in frame I) in the myxoma. I. S indicates the string that suspended the myxoma in the water bath. This study suggests that, in the absence of calcification, a very hyperrefractile mass may be a lipoma rather than a myxoma. LA, left atrium; LV, left ventricle; M, myxoma; RA, right atrium; RV, right ventricle; T, transverse plane. (A,B, and G through I reproduced with permission from Mehta R, Nanda NC, Osman K, et al. Left ventricular lipoma by transesophageal and in vitro echocardiographic studies. Echocardiography 1995;12:283–288. ) |
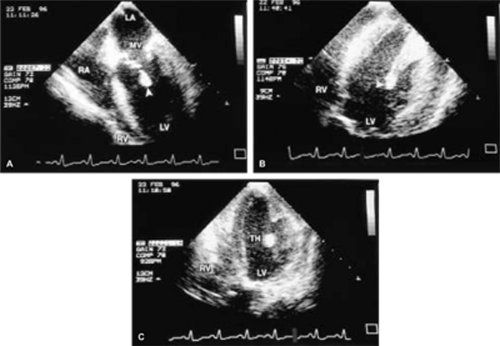 FIGURE 9.14. Left ventricular thrombus. A–C. A mass (arrowheads) attached to a papillary muscle in the left ventricle (LV) in a patient with aortic stenosis. This mass was found to be a thrombus (TH) at surgery. LA, left atrium; MV, mitral valve; RA, right atrium; RV, right ventricle. |
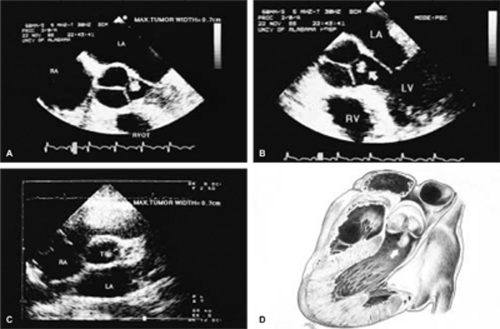 FIGURE 9.15. Aortic valve fibroelastoma. A small irregular mass (arrow in B, transverse plane [T]) in C) is seen attached to the left coronary leaflet of the aortic valve (AV) by a short stalk (A). There was no clinical evidence of endocarditis or significant aortic regurgitation (AR) in this patient. The mass was resected and found to be a fibroelastoma. D. Schematic shows a fibroelastoma. LA, left atrium; LV, left ventricle; RA, right atrium; RVOT, right ventricular outflow tract. |
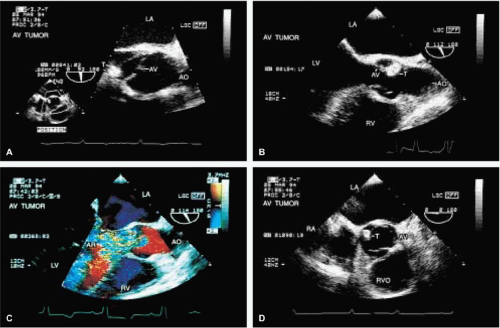 FIGURE 9.16. Aortic valve mass. A–D. The mass-like lesion (T) attached to the noncoronary cusp of the aortic valve (AV) in this patient mimics a tumor but is actually a vegetation with typical clinical findings of endocarditis. Note associated severe AR (C). AO, aorta; AR, aortic regurgitation; LA, left atrium; LV, left ventricle; RA, right atrium; RV, right ventricle; RVO, right ventricular outflow. |
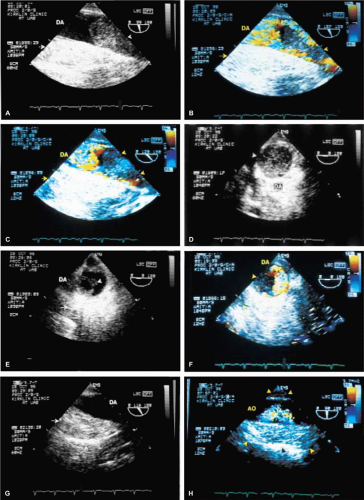 FIGURE 9.17. Aortic leiomyosarcoma. A–F. A mass (arrowheads) in the descending thoracic aorta (DA). Color Doppler examination shows prominent flow signals in the unobstructed portion of the aorta (AO). This makes thrombus unlikely, because associated spontaneous contrast echoes caused by a low-flow state usually are present. Also, no dissection flap is identified. The arrows in A through C and E through H show a large echogenic mass outside the aorta, consistent with hematoma. G,H. A hematoma (arrow, arrowheads) is seen extending on both sides of the descending aorta (DA, AO), even where the tumor mass is not present. At surgery, the mass was found to be a leiomyosarcoma that involved the aortic wall, resulting in perforation that caused the hematoma. |
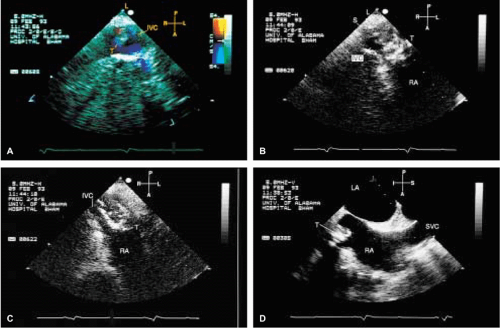 FIGURE 9.18. Primary leiomyoma of the inferior vena cava. A,B. The subcostal transverse planes show the large tumor mass (T) clearly attached (S) in the inferior vena cava (IVC). B,C. The portion of the tumor protruding into the right atrium (RA) is highly echogenic, indicative of calcific involvement, whereas the IVC portion has very few highly refractile echo densities, suggesting paucity of calcific deposits. D. Longitudinal plane examination also demonstrates the tumor (T) protruding into the RA. L, liver; LA, left atrium; SVC, superior vena cava. (Reproduced with permission from Loungani RR, Nanda NC, Sanyal RS, et al. Transesophageal echocardiographic findings in primary leiomyoma of inferior vena cava. Echocardiography 1993;10:623–627. ) |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


