Fig. 11.1
Huge splenic artery false aneurysm opened in a pseudocyst, discovered 6 m after an acute pancreatitis. (a) CT: Large pseudoaneurysm opened in a pseudocyst. (b) Selective injection of the splenic artery: slow enhancement of this voluminous hilar lesion. (c) Coiling upstream of the lesion and immediately downstream of a collateral branch independent of this false aneurysm, feeding the superior pole of the spleen parenchyma. (d) CT 1 month later: excluded false aneurysm, large hypodense splenic parenchymous area, but remaining consequent enhanced parenchyma
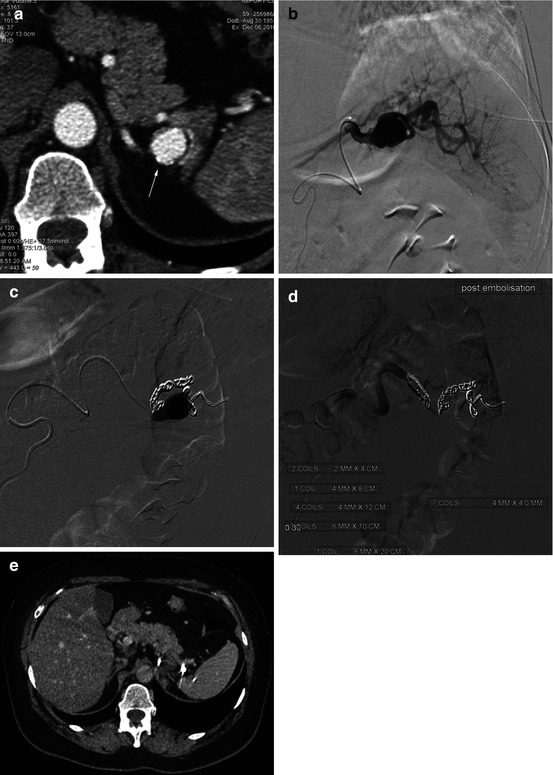
Fig. 11.2
Asymptomatic 18 mm diameter sacciform splenic artery aneurysm. (a) CT: diagnosis of a splenic artery aneurysm (arrow). (b) Hyperselective splenic artery injection (microcatheter): aneurysm, with two efferent branches. (c) Catheterization and coiling of the branches downstream to the aneurysm (d) and then upstream coiling, leading to a “sandwich” exclusion (upstream + downstream). (e) CT 1 m later: correct splenic parenchymal enhancement via the gastric arteries collateral feeding
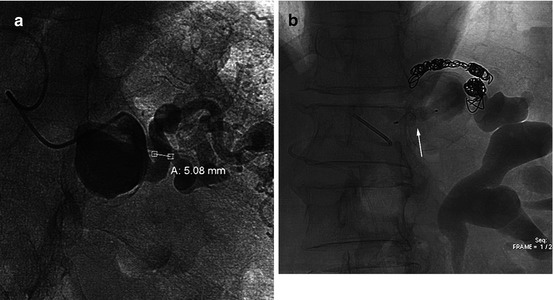
Fig. 11.3
A 65-year-old W, asymptomatic 35 mm truncal SA aneurysm, discovered on a CT. (a) Selective SA arteriography: two efferent arteries. (b) Control angio after sandwich exclusion: downstream (coiling of two efferent branches) and upstream (truncal AVP, arrow)
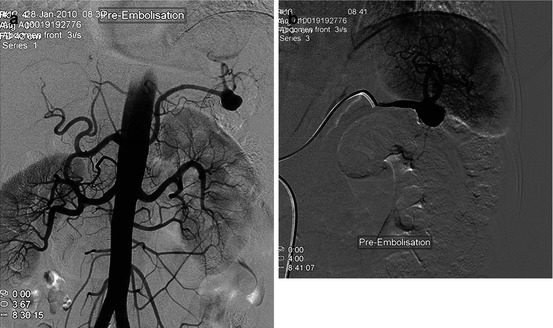
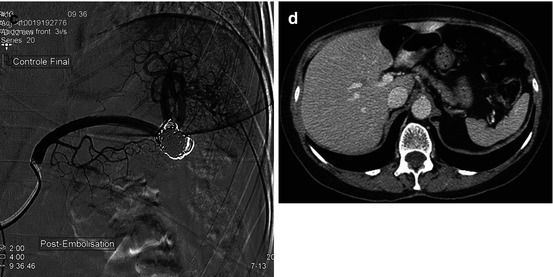
Fig. 11.4
(a) Asymptomatic CT diagnosed sacciform SA 30 mm aneurysm: aortography. (b) Selective arteriography: large neck aneurysm, located at the end of the SA trunk. (c) Control angio after coil packing. (d) CT 1 month later: correct splenic parenchyma enhancement
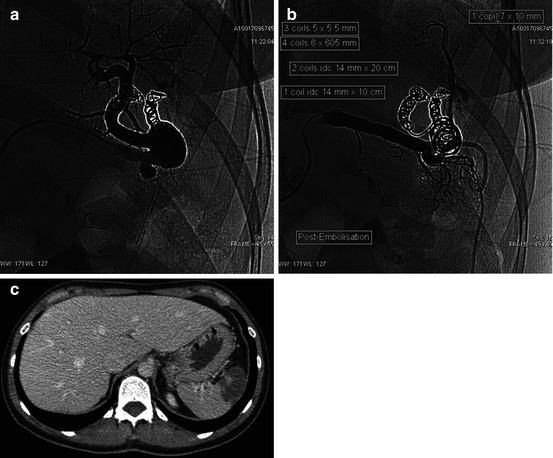
Fig. 11.5
Huge asymptomatic splenic artery aneurysm. (a) Efferent branches coil exclusion (b) and then packing of the sac. (c) CT 1 month later: partial splenic infarction
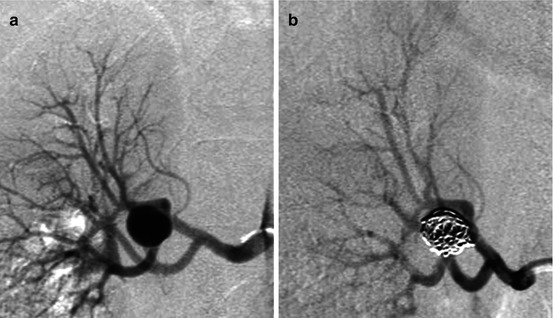
Fig. 11.6




Sacciform aneurysm of the inferior first-order branch of the right prepyelic renal A (Rundback type II). (a) Selective arteriography. (b) Angiographic control after packing
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
