38 Tricuspid and Pulmonic Valve Disease
Tricuspid Stenosis
Etiology, Pathogenesis, and Differential Diagnosis
Tricuspid stenosis is uncommon. Most cases are due to rheumatic heart disease. When rheumatic tricuspid stenosis is present, it is generally associated with mitral stenosis, which usually accounts for most of the presenting signs and symptoms. Carcinoid heart disease may also cause tricuspid stenosis, and the signs and symptoms may be mimicked by tumors (myxoma or metastasis), or vegetations that obstruct right ventricular (RV) inflow, particularly those associated with pacemaker leads (Box 38-1).
Clinical Presentation
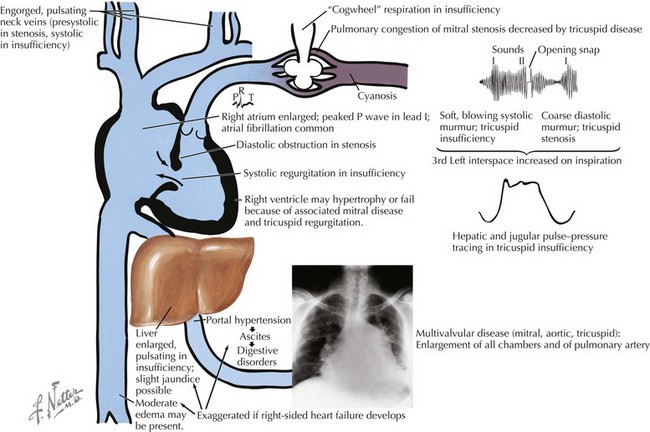
The symptoms of tricuspid stenosis are mainly due to increased systemic venous pressure that results from a hemodynamically significant tricuspid valve lesion (Fig. 38-1). Peripheral edema, ascites, hepatic enlargement, and right upper quadrant discomfort may develop with chronic tricuspid stenosis or regurgitation. Decreased cardiac output may cause pronounced fatigue, and an occasional patient will complain of the appearance or sensation of the prominent a wave in the jugular veins, which results from increased jugular venous pressure due to impaired RV filling during atrial systole. The murmur of tricuspid stenosis is a low-pitched diastolic murmur at the lower left sternal edge. However, this is often obscured by or difficult to differentiate from the usually associated mitral stenosis murmur. The physical examination, however, may demonstrate the presence of tricuspid stenosis in patients with mitral stenosis, including when there is accentuation of the diastolic murmur during inspiration (as is the case for most right-sided murmurs), a prominent a wave in the jugular venous pulse, or both. An opening snap is occasionally appreciated but may be difficult to distinguish from that of coexistent mitral stenosis. When appreciated, it is usually heard following and more medial to the mitral opening snap.
Diagnostic Approach
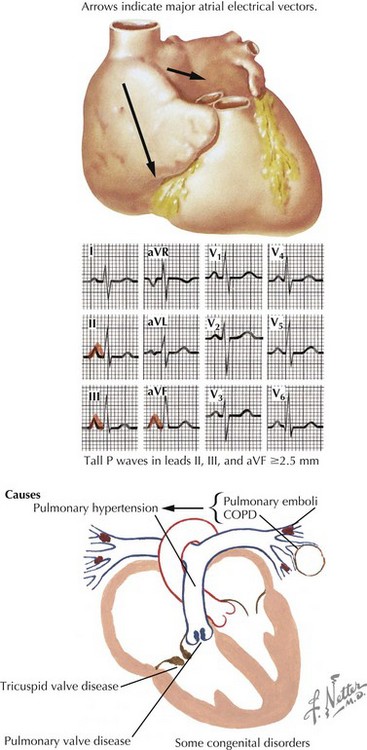
Useful diagnostic studies include chest radiography, ECG, and echocardiography with Doppler evaluation. Right atrial (RA) enlargement is frequently evident on radiographs and is manifest on the ECG as a large peaked P wave in lead II (Fig. 38-2). Because of the increased RA pressure, atrial fibrillation is often present.